Névrome de Morton
Revu par Dr Surangi Mendis, MRCGPDernière mise à jour par Dr Philippa Vincent, MRCGPDernière mise à jour 10 août 2023
Respecte les directives éditoriales
- TéléchargerTélécharger
- Partager
- Language
- Discussion
- Version audio
- Ajouter aux sources préférées sur Google
Dans cette série :Fasciite plantaireTendinopathie d'AchilleRupture du tendon d'AchilleMétatarsalgieFractures métatarsiennesPieds plats et voûtes plantaires affaissées
Morton's neuroma is a condition that affects one of the nerves that run between the long bones (metatarsals) in the foot. The exact cause is not certain.
Symptoms include pain, burning, numbness and tingling between two of the toes of the foot. About a third of cases resolve withd simple treatments including modification of footwear. Sometimes surgery is needed for long-standing (chronic) symptoms.
En un coup d'œil
Morton's neuroma is a thickening of a nerve in the foot, usually between the third and fourth toes.
It causes pain, numbness, burning, and tingling in the affected toes.
Symptoms are often worse with high-heeled or narrow shoes, and better with rest.
It is thought to be caused by long-standing stress and irritation of the nerve.
Treatment includes wearing comfortable, wide shoes and using special shoe inserts.
If non-surgical treatments don't work, injections or surgery may be options.
See a doctor if pain lasts for three months despite changing footwear and using insoles.
What is Morton's neuroma?
Morton's neuroma is named after Dr Morton who first described this condition in 1876. It is sometimes called Morton's metatarsalgia or interdigital neuroma.
It is a condition that affects one of the common plantar digital nerves that run between the long bones (metatarsals) in the foot. It most commonly affects the nerve between the third and fourth metatarsal bones, causing pain and numbness in the third and fourth toes.
It can also affect the nerve between the second and third metatarsal bones, causing symptoms in the second and third toes. Morton's neuroma rarely affects the nerve between the first and second, or between the fourth and fifth, metatarsal bones. It tends to affect only one foot and it is rare to have two neuromas at the same time in the same foot.
What causes Morton's neuroma?
Despite its name, Morton's neuroma is not actually a neuroma.
A neuroma is a non-cancerous (benign) tumour that grows from the fibrous coverings of a nerve. There is no tumour formation in Morton's neuroma. Instead, there is a thickening of the nerve.
The exact cause of Morton's neuroma is not known. It is thought to develop as a result of long-standing (chronic) stress and irritation of a plantar digital nerve.
This may be due to the nerve being squashed (compressed), rubbed or stretched. Some thickening (fibrosis) and swelling may then develop around a part of the nerve. This can look like a neuroma and can lead to compression of the nerve.
The anatomy of the bones of the foot is also thought to contribute to the development of Morton's neuroma. The space between the long bones (metatarsals) in the foot is narrower between the second and third and between the third and fourth metatarsals. This means that the nerves that run between these metatarsals are more likely to be compressed and irritated. Wearing narrow shoes can make this compression worse.
Sometimes, other problems can contribute to the compression of the nerve. These include the growth of a fatty lump (called a lipome) and also the formation of a fluid-filled sac that can form around a joint (a bursa).
Also, inflammation in the joints in the foot next to one of the digital nerves can sometimes cause irritation of the nerve and lead to the symptoms of Morton's neuroma.
Morton's neuroma symptoms
People with Morton's neuroma usually complain of pain that can start in the ball of the foot and shoot into the affected toes. Some people just have toe pain. There may also be burning and tingling of the toes. Some people describe the pain that they feel as being like walking on a stone or a marble.
Symptoms can be made worse if wearing high-heeled shoes. The pain can be relieved by taking the shoe off, resting your foot and massaging the area. There may also be some numbness between the affected toes.
The symptoms can vary and may come and go over a number of years. For example, some people may experience two attacks of pain in a week and then nothing for a year. Others may have regular and persistent (chronic) pain.
Quand consulter un médecin
It is sensible to seek medical advice if the pain has been persistent for three months, despite changing footwear and buying inner soles to try and help the problem. A podiatry referral is likely to be advised at that stage.
Who develops Morton's neuroma?
About three people out of four who have Morton's neuroma are women. It most commonly affects people between the ages of 40 and 60 but can occur at any age.
Poorly fitting or constricting shoes can contribute to Morton's neuroma. It is more common in women who habitually wear high-heeled shoes or in men who are required to wear tight (constrictive) footwear. It may also be more common in ballet dancers and runners. In some people there is no obvious cause.
How is Morton's neuroma diagnosed?
Morton's neuroma is usually diagnosed by a clinician listening to the symptoms and examining the foot. Sometimes a doctor can feel the 'neuroma', or an area of thickening in your foot, which may be tender. Pressing on the area between the long bones in your foot may show a tender spot.
Occasionally a clinician may suggest an échographie ou IRM to confirm the diagnosis but this is rarely necessary. Occasionally, other tests such as analyses de sang ou un radiographie may be needed to rule out other conditions.
What is the treatment for Morton's neuroma?
Non-surgical treatments
Non-surgical treatments may be all that are needed for many people with a Morton's neuroma. From the simple to the more technical, they include the following:
Choosing the right footwear is very important. It is important to avoid high-heeled and narrow or pointed-toe shoes, as well as shoes with thin soles. Wearing comfortable, wide-fitting shoes which don't squash the feet is best.
Pads inside the shoes are often helpful. Shoe inserts (also called orthoses) for this condition can be bought in pharmacies over the counter. To protect the nerve, metatarsal pad can be obtained - this is a soft pad which sits below the ball of the foot. . It should fit behind the ball of the foot, rather than directly underneath it. Insoles with metatarsal domes may also be effective. These are cushions for the whole foot, with a raised dome-like area under the ball of your foot.
Stéroïde or local anaesthetic injections (or a combination of both) into the affected area of the foot may be needed if the simple footwear changes do not fully relieve symptoms. This may be done by a specialist in ultrasound scans (radiologist) who injects whilst doing the ultrasound scan. It may also be done by a podiatrist or an orthopaedic surgeon. This has been shown to give good pain relief, at least in the short term. However, the footwear modification measures should still be continued.
Manipulation/mobilisation has been found to be effective in some cases.
Sclerosant injections involve the injection of alcohol and local anaesthetic into the affected nerve under the guidance of an ultrasound scan. Some studies have shown this to be as effective as surgery. However, this is not widely available in the UK yet.
Freezing (cryotherapy) is sometimes used but is not widely available in the UK.
Ablation par radiofréquence is another treatment which has been studied. This involves treating the nerve with heat energy waves. It is not yet proven how effective this is.
Traitements chirurgicaux
If these non-surgical measures do not work, an operation is sometimes needed. Surgery normally involves a small cut (incision) being made on either the top or the sole of the foot, between the affected toes. The surgeon will cut out (resect) the affected nerve. Alternatively, the surgeon may create more space around the affected nerve (known as nerve decompression). If the nerve is resected, there will be some permanent numbness of the skin between the affected toes. This does not usually cause any problems.
A special shoe is usually needed for a short time after surgery until the wound has healed and normal footwear can be used again.
At least three quarters of people have a satisfactory result from surgery. As with any surgical operation, there is a small risk of complications. For example, after this operation a small number of people can develop a wound infection. Painful scars occur in about 5 out of 100 people after surgery. A small but significant number of people report that their pain is worse after surgery.
What is the outlook for Morton's neuroma?
About one third of people with Morton's neuroma get better just with changing their footwear and using metatarsal pads. Of those who choose to have surgery, about three out of four will have good results with relief of their symptoms.
Recurrent or persisting (chronic) symptoms can occur after surgery. Sometimes, decompression of the nerve may have been incomplete or the nerve may just remain 'irritable'.
In those who have had cutting out (resection) of the nerve (neurectomy), a recurrent or 'stump' neuroma may develop in any nerve tissue that was left behind. This can itself be very painful. In one in four people who have got better with an operation, the problem returns at a later date. It is important to keep wearing the right shoes to prevent this from happening.
Can Morton's neuroma be prevented?
Ensuring that shoes are well fitted, low-heeled and with a wide toe area may help to prevent Morton's neuroma.
Some anatomy of the foot
There are many bones in the foot. They can briefly be divided into the tarsal bones, the long bones (metatarsals) and the phalanges. The tarsal bones are the larger bones that form the back section of the foot, with the calcaneum being the largest.
There are five metatarsal bones and these are given names from the first to the fifth. The first metatarsal bone is the largest and is the bone that joins to the big toe. Each toe has three phalanges, except the big toe which only has two.
Névrome de Morton
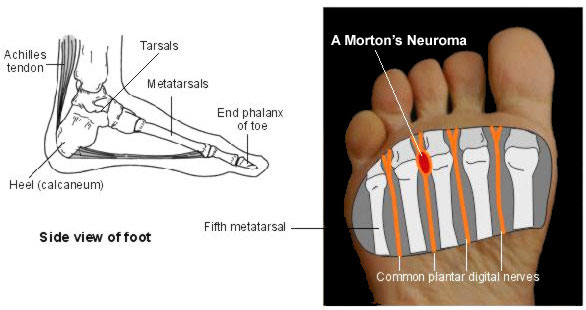
There are many nerves, muscles and ligaments within the foot. Of note, the common plantar digital nerves run between the metatarsal bones in the foot. These have branches that supply sensation to the skin of the toes.
Sélections des patients pour Douleur au talon et au pied

Soin des pieds
Maladie de Sever
La maladie de Sever (parfois appelée apophysite calcanéenne) provoque des douleurs au talon. Elle est plus fréquente chez les enfants qui participent régulièrement à des activités sportives à fort impact, comme la course et le saut. Elle peut généralement être traitée par du repos, le port de chaussures de sport de soutien et des semelles pour soutenir le talon. C'est une affection bénigne qui s'améliore généralement en quelques semaines ou quelques mois.
par Dr Hayley Willacy, FRCGP

Soin des pieds
Fasciite plantaire
Les douleurs au talon et au pied sont très courantes. Une cause fréquente est la fasciite plantaire, qui provoque une douleur sous le talon. Elle disparaît généralement avec le temps, mais différents traitements peuvent aider.
par Dr Surangi Mendis, MRCGP
Questions fréquemment posées
Can Morton's neuroma affect multiple toes at once?
Morton's neuroma most commonly affects the nerve between the third and fourth metatarsal bones, causing pain and numbness in the third and fourth toes. It can also affect the nerve between the second and third metatarsal bones, leading to symptoms in the second and third toes. It rarely affects nerves connecting the first and second, or fourth and fifth, metatarsal bones. It usually affects only one foot and it's uncommon to have two neuromas in the same foot at the same time.
Is Morton's neuroma a cancerous growth?
Despite its name, Moreton's neuroma is not actually a neuroma in the sense of a non-cancerous (benign) tumour that grows from nerve coverings. Instead, it involves a thickening of the nerve without tumour formation.
Are there certain activities that make Morton's neuroma more likely?
Morton's neuroma is more common in women, particularly those who regularly wear high-heeled shoes. Men who wear tight or constrictive footwear can also be affected. It may also be more prevalent among ballet dancers and runners. In some cases, there is no obvious cause.
How can I tell if my foot pain is Morton's neuroma or something else?
Morton's neuroma typically causes pain that starts in the ball of the foot and can shoot into the affected toes. There might also be burning, tingling, or numbness between these toes. Some people describe the sensation as if they are walking on a stone or marble. However, other tests like blood tests or X-rays might sometimes be needed to rule out other conditions causing similar symptoms.
Can wearing orthotics or shoe inserts help with Morton's neuroma?
Yes, pads inside shoes, also known as orthoses, can often be helpful. These include metatarsal pads, which are soft pads placed behind the ball of the foot, and insoles with metatarsal domes that provide cushioning for the whole foot with a raised area under the ball of the foot. These can be bought over-the-counter in pharmacies.
How long does it take for non-surgical treatments to work for Morton's neuroma?
The article indicates that steroid or local anaesthetic injections can give good short-term pain relief, but doesn't specify a timeframe for other non-surgical treatments to show results. It does mention that if pain persists for three months despite changing footwear and using insoles, it's sensible to seek medical advice.
Lectures complémentaires et références
- Morton's Neuroma: Interdigital Perineural Fibrosis; Manuel d'Orthopédie de Wheeless
- Musson RE, Sawhney JS, Lamb L, et al; Ultrasound guided alcohol ablation of Morton's neuroma. Foot Ankle Int. 2012 Mar;33(3):196-201.
- Makki D, Haddad BZ, Mahmood Z, et al; Efficacy of corticosteroid injection versus size of plantar interdigital neuroma. Foot Ankle Int. 2012 Sep;33(9):722-6.
- Radiofrequency ablation for symptomatic interdigital (Morton’s) neuroma; NICE Interventional Procedure Guidance, December 2015
- Matthews BG, Hurn SE, Harding MP, et al; The effectiveness of non-surgical interventions for common plantar digital compressive neuropathy (Morton's neuroma): a systematic review and meta-analysis. J Foot Ankle Res. 2019 Feb 13;12:12. doi: 10.1186/s13047-019-0320-7. eCollection 2019.
- Munir U, Tafti D, Morgan S; Morton Neuroma.
- Névrome de Morton; NICE CKS, novembre 2021 (accès réservé au Royaume-Uni)
À propos de l'auteurVoir la biographie complète

Dr Philippa Vincent, MRCGP
Médecin généraliste, Auteur médical
MB BS, Bsc, MRCGP (2000), DCH, DFSRH, DRCOG
Dr Philippa Vincent est un médecin généraliste du NHS travaillant dans le nord de Londres.
À propos du critiqueVoir la biographie complète

Dr Surangi Mendis, MRCGP
Consultant and Medical Author
MBBS, BSc (1st), MRCGP (2014), DFSRH, PGcert otology and audiology
Surangi Mendis is a consultant in Audiovestibular Medicine and Neuro-otology at The Royal National ENT and Eastman Dental Hospitals, UCLH.
Historique de l'article
Les informations sur cette page sont rédigées et examinées par des cliniciens qualifiés.
Article également disponible en Anglais, Allemand, Espagnol, Français, Italien, Portugais, Hindi, Hébreu, Arabe, and Suédois.
Prochaine révision prévue : 8 août 2028
10 août 2023 | Dernière version

Demandez, partagez, connectez-vous.
Parcourez les discussions, posez des questions et partagez vos expériences sur des centaines de sujets de santé.

Vous ne vous sentez pas bien ?
Évaluez vos symptômes en ligne gratuitement
Inscrivez-vous à la newsletter Patient
Votre dose hebdomadaire de conseils de santé clairs et fiables - rédigés pour vous aider à vous sentir informé, confiant et maître de la situation.
En vous abonnant, vous acceptez notre Politique de confidentialité. Vous pouvez vous désabonner à tout moment. Nous ne vendons jamais vos données.
Plus de soins des pieds
- Tendinopathie d'Achille
- Pieds vieillissants
- Blessure à la cheville
- Pied d'athlète
- Orteil cassé
- Hallux valgus
- Pied bot
- Cors et callosités
- Ulcères du pied diabétique
- Pieds plats et voûtes plantaires affaissées
- Ampoules aux pieds
- Infection fongique des ongles
- Ongle incarné
- Fractures métatarsiennes
- Métatarsalgie
- Psoriasis des ongles
- Fasciite plantaire
- Pédicurie
- Pieds moites
- Verrues et verrues plantaires