Scoliose et cyphose
Curvature of the spine
Revu par Dr Hayley Willacy, FRCGP Dernière mise à jour par Dr Colin Tidy, MRCGPDernière mise à jour 16 mars 2023
Respecte les directives éditoriales
- TéléchargerTélécharger
- Partager
- Language
- Discussion
- Version audio
- Ajouter aux sources préférées sur Google
La scoliose est une affection du dos qui provoque une courbure latérale de la colonne vertébrale - soit à gauche, soit à droite. La plupart des cas se développent chez les enfants âgés de 9 à 14 ans pendant la poussée de croissance de la puberté. La scoliose est généralement légère et ne nécessite aucun traitement. Pour les cas plus graves, les traitements incluent des exercices spécifiques, un corset dorsal ou, occasionnellement, une chirurgie pour redresser la colonne vertébrale. Une courbure très prononcée d'avant en arrière est appelée cyphose, qui ne nécessite généralement pas de traitement.
En un coup d'œil
Scoliosis is a sideways curve of the spine.
La courbure peut être légère ou sévère, et dans différentes parties de la colonne vertébrale.
La plupart des cas de scoliose n'ont pas de cause connue et apparaissent souvent pendant la puberté.
Les symptômes peuvent inclure un dos bombé lors de la flexion ou des épaules/hanches inégales.
La surveillance régulière, la physiothérapie, un corset dorsal ou la chirurgie peuvent être des options de traitement.
What is scoliosis?
La scoliose
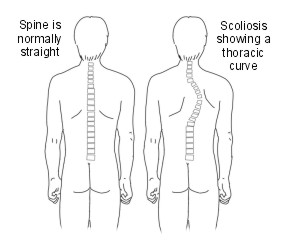
The word scoliosis comes from the Greek word meaning crooked. The back (spine) should look straight, up and down, when you look at someone from behind. If the spine has a sideways curve, it is called a scoliosis.
The curve can bend to the left or to the right. The severity of the curve can vary from very mild and barely noticeable to severe.
The curve can be in the lower part of the spine (a lumbar curve), in the upper part of the spine (a thoracic curve) or go from the upper to lower part of the spine (a thoracolumbar curve). In some cases there is a double curve - like an S shape.
What is the difference between scoliosis and kyphosis?
If you look at someone from the side, normally there are three slight front-to-back curves in the spine - one in the neck, one in the chest section and one in the lower back. An abnormal, more pronounced front-to-back curve is called a kyphosis. This is different to a scoliosis which isn't noticeable from the side.
What are the causes of kyphosis?
Kyphosis can occur at any age, although it is rare at birth. Adolescent kyphosis, is known as Scheuermann's disease.This type of kyphosis is caused by the wedging together in a row of several bones (vertebrae) of the back (spine). The cause of Scheuermann's disease is unknown.
In adults, various conditions affecting the spine can cause a higher risk of kyphosis, including:
Arthrite of the spine.
'Amincissement' des os (ostéoporose) of the spine, if it has caused one or more of the bones in the spine to flatten (called a wedge-shaped fracture).
The treatment usually depends on the underlying cause. This is covered in the separate leaflets on those specific subjects - follow links in red.
What causes scoliosis?
There are several different types of scoliosis and the causes of each are different:
Non-structural scoliosis (functional or postural scoliosis)
In this type, the back (spine) is structurally normal, but looks curved because of another condition such as having one leg that is significantly longer than the other or muscle spasm in the back muscles. The curve is usually mild and it changes or goes away when the person bends sideways or forwards.
Structural scoliosis
In these cases, the curve is fixed and doesn't go away when the person changes position. There are different types:
Idiopathic. This means the cause is not known. For more than 8 out of every 10 people with scoliosis the cause is idiopathic.
Neuromuscular scoliosis. This means the curve is caused by a condition which affects muscles or nerves of the back. For example, it may happen in some people with dystrophie musculaire, polio, la paralysie cérébrale, or neurofibromatosis. Each of these conditions has other symptoms and problems in addition to a scoliosis. In around 1 out of every 10 people with scoliosis it is due to a neuromuscular problem.
Osteopathic. This means as a result of a bone abnormality.
Congenital scoliosis. This means the spine has not formed properly while the person was a baby developing in the womb. Around 1 in every 10 people with scoliosis have had it since birth.
The rest of this leaflet is about the most common type - idiopathic scoliosis.
Who develops idiopathic scoliosis?
Idiopathic scoliosis can develop at any stage in childhood. It is not known how or why it develops. It is pas due to poor posture and you cannot prevent it starting.
It most commonly develops during the growth spurt of puberty and early adolescence. This is usually between the ages of 10-12 years for girls and 11-16 years for boys. About 1 in 40 children have some degree of scoliosis. Mild scoliosis affects about the same number of boys and girls. However, moderate or severe scoliosis is more common in girls.
Idiopathic scoliosis is not a straightforward hereditary condition. However, about 1 out of every 4 people affected with scoliosis have one or more other family members with the same condition.
Idiopathic scoliosis symptoms
In most cases the onset of the scoliosis is gradual and painless. Scoliosis is usually noticeable on bending down. Sometimes a mild-to-moderate scoliosis can develop without being noticed by the child or their parent/s. This is often because the condition usually develops during adolescence when children often become more self-conscious. Parents and others are less likely then to see a naked back (spine) and see the problem.
Scoliosis can cause mild pain and imbalance of the muscles. If scoliosis becomes more severe then it can become more disfiguring. This is because when the spine curves sideways, as the curve becomes more severe, the small bones (vertebrae) that make up the spine also twist around. This pulls any attached muscles, ligaments and ribs around with them. As a consequence:
If the scoliosis is in the chest (thoracic) region, the ribs and shoulder blades stick out like a bulge on one side of the back. Also, one shoulder may hang lower than the other and one shoulder blade may be higher than the other.
If the scoliosis is in the lower back (lumbar) region, it can make the pelvis thrust forward on one side and one leg may appear to be shorter than the other.
If scoliosis is not treated and becomes severe, it can cause problems later in life. For example, persistent back pain may develop and it can affect your general fitness and your overall quality of life. If the deformity is very severe, breathing problems or heart problems may develop - this is fortunately rare.
If a child has back pain it is very unlikely that it is due to scoliosis. For more common causes of children's back pain, see the separate leaflet called Back Pain in Children.
How is idiopathic scoliosis diagnosed?
Scoliosis diagnosis
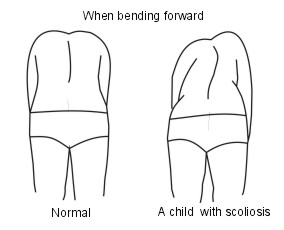
Scoliosis is often seen when you bend forward. A bulge on the back (spine) is more obvious when bending forward.
If your doctor diagnoses scoliosis then you will usually be referred to a specialist.
X-ray pictures of the back are sometimes done to assess the angle of the curve. This gives an idea of the severity of the condition and the likelihood of it getting worse. Other investigations - for example, magnetic resonance imaging (MRI) scanning ou computerised tomography (CT) scanning of the neck - are needed in some cases.
What is the treatment for idiopathic scoliosis?
The aims of treating scoliosis are:
To prevent the curve becoming worse.
To avoid the need for surgery in later life.
To prevent breathing problems.
To improve how the spine looks.
People with more severe scoliosis may need treatment to stabilise the back (spine). Many people with scoliosis do not need treatment.
Treatment depends on various factors, such as:
The person's age.
Whether they are female or male - scoliosis in girls tends to worsen more quickly.
Whether they are still growing.
The severity of the curve.
The exact location of the scoliosis - for example, the upper (thoracic) or lower (lumbar) back.
The chance that scoliosis may progress.
Treatment options include observation, specific physiotherapy exercises, wearing a brace, and surgery. The international Scientific Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) recommend that non-surgical treatment should be delivered by a specialist team to include a doctor, physiotherapist, orthotist and possibly also a psychologist.
Observation
Most people have mild scoliosis and do not need any treatment. However, a specialist may arrange regular reviews to make sure that the scoliosis is not getting worse as children get older. Once the main bone growth ends after puberty, scoliosis does not usually worsen.
Sports and other activities can be done normally - there is some evidence that sport and exercise make people with scoliosis feel better about themselves and that they have fewer emotional problems. Occasionally, a specialist may advise against certain activities such as heavy contact sports or gymnastics.
Physiothérapie
Research that shows that specific exercises help to prevent scoliosis worsening has recently been published. The exercises are called physiotherapeutic scoliosis specific exercises (PSSE) and need to be performed from twice a week to daily and occasionally several times a day. This requires a lot of motivation.
Back braces
There are several different types of back brace. The more modern ones are more comfortable to wear than the older ones. If the scoliosis is moderate or becoming worse, then a back brace may be advised, either alone or in addition to PSSE. A brace does not cure a scoliosis. The aim of a brace is to prevent the scoliosis from becoming worse as the child grows. A brace is worn most of the day and night.
Towards the end of treatment they often only need to be worn at night. Most normal activities can be done whilst wearing a back brace. However, they need to be removed for washing and swimming. Wearing a back brace can be difficult for a young person to stick to. An expert team will involve them in the decision to wear a brace, so that they understand why they are doing it and what they are going to gain from it - if it isn't worn, it won't work.
Chirurgie
An operation is sometimes advised for people with severe scoliosis, although if a brace is worn it should be possible to prevent the need for surgery. The aim of the operation is to correct the curve, to stabilise the spine and also to fuse the curve. Spinal fusion is the joining of two or more back bones (vertebrae). Implants or rods are often used to keep the back straight after the operation. These rods are usually lengthened every 4-6 months as you grow.
There are different surgical techniques used. Your specialist will be able to advise which type of surgery, if any, may be beneficial for you. In general, the operations done for scoliosis are usually very long procedures and involve many months of recovery afterwards. Also, they are not always successful.
Traitements alternatifs
There is good-quality research that has shown that osteopathy does not help to resolve or improve scoliosis. There is also no reliable evidence that other techniques, such as chiropractic, reflexology, acupuncture, neurostimulation, are effective. However, some people with scoliosis find one or more of these complementary therapies to be useful to improve backache or pain.
Sélections des patients pour Troubles du cou et de la colonne vertébrale

Os, articulations et muscles
Douleur au dos et à la colonne vertébrale
Les douleurs dorsales sont extrêmement courantes ; la plupart d'entre nous en souffriront à un moment donné. Les enfants peuvent avoir des douleurs dorsales, mais elles sont plus fréquentes chez les adultes. Ce dépliant fournit des informations générales sur le dos et les douleurs dorsales. Il vous dirigera également vers des pages contenant des informations plus détaillées sur les différentes affections pouvant causer des douleurs dorsales.
par Dr Toni Hazell, MRCGP

Os, articulations et muscles
Problèmes de disques vertébraux
Les disques vertébraux sont également appelés disques intervertébraux. Il y a un disque entre chaque os (vertèbre) de votre colonne vertébrale. Cela maintient les vertèbres séparées et sert d'amortisseur. En vieillissant, les disques vertébraux se détériorent progressivement, ce qui peut entraîner des problèmes tels que des douleurs dorsales. D'autres problèmes affectant les disques vertébraux incluent une hernie discale ou, beaucoup plus rarement, une infection (discite).
par Dr Hayley Willacy, FRCGP
Questions fréquemment posées
Can poor posture cause scoliosis?
Non, la scoliose idiopathique, le type le plus courant, n'est pas causée par une mauvaise posture. Elle ne peut pas non plus être évitée en améliorant consciemment la posture.
Est-il normal que la scoliose provoque des douleurs ?
La scoliose commence généralement de manière progressive et indolore. Bien qu'elle puisse causer une douleur légère et un déséquilibre musculaire, il est très peu probable que les douleurs dorsales chez les enfants soient causées par la scoliose. Si la condition devient sévère, des douleurs dorsales persistantes peuvent se développer plus tard dans la vie.
Quelle est la fréquence de la scoliose idiopathique chez les enfants ?
Environ 1 enfant sur 40 présente un certain degré de scoliose. La scoliose légère affecte les garçons et les filles de manière égale, mais les cas modérés ou sévères sont plus fréquents chez les filles.
Existe-t-il des thérapies alternatives qui peuvent guérir ou améliorer la scoliose ?
La recherche a montré que l'ostéopathie n'aide pas à résoudre ou à améliorer la scoliose. Il n'existe pas non plus de preuves fiables que d'autres techniques comme la chiropractie, la réflexologie, l'acupuncture ou la neurostimulation soient efficaces pour traiter la condition elle-même. Cependant, certaines personnes trouvent ces thérapies complémentaires utiles pour gérer les maux de dos ou la douleur associée à la scoliose.
Ma scoliose va-t-elle s'aggraver après la puberté ?
Pour la plupart des gens, une fois que la croissance osseuse principale se termine après la puberté, la scoliose idiopathique ne s'aggrave généralement pas.
Lectures complémentaires et références
- Monticone M, Ambrosini E, Cazzaniga D, et al; L'auto-correction active et les exercices orientés vers la tâche réduisent la déformation de la colonne vertébrale et améliorent la qualité de vie chez les sujets atteints de scoliose idiopathique légère de l'adolescent. Résultats d'une étude contrôlée randomisée. Eur Spine J. 2014 juin; 23(6): 1204-14. doi : 10.1007/s00586-014-3241-y. Epub 2014 28 février.
- Theis J, Gerdhem P, Abbott A; Résultats sur la qualité de vie chez les patients adultes atteints de scoliose opérés : une revue systématique. Eur Spine J. 2014 Nov 8.
- Negrini S, Minozzi S, Bettany-Saltikov J, et al; Corsets pour la scoliose idiopathique chez les adolescents. Cochrane Database Syst Rev. 2015 Jun 18;(6):CD006850. doi: 10.1002/14651858.CD006850.pub3.
- Negrini S, Donzelli S, Aulisa AG, et al; 2016 Lignes directrices SOSORT : traitement orthopédique et de rééducation de la scoliose idiopathique pendant la croissance. Scoliosis Spinal Disord. 2018 Jan 10;13:3. doi : 10.1186/s13013-017-0145-8. Collection électronique 2018.
- Bettany-Saltikov J, Turnbull D, Ng SY, et al; Management of Spinal Deformities and Evidence of Treatment Effectiveness. Open Orthop J. 2017 Dec 29;11:1521-1547. doi: 10.2174/1874325001711011521. eCollection 2017.
- Ali A, Fontanari V, Fontana M, et al; Spinal Deformities and Advancement in Corrective Orthoses. Bioengineering (Basel). 2020 Dec 25;8(1):2. doi: 10.3390/bioengineering8010002.
- Smith JS, Shaffrey CI, Ames CP, et al; Treatment of adult thoracolumbar spinal deformity: past, present, and future. J Neurosurg Spine. 2019 May 1;30(5):551-567. doi: 10.3171/2019.1.SPINE181494.
À propos de l'auteurVoir la biographie complète

Dr Colin Tidy, MRCGP
Médecin généraliste, Auteur médical
MBBS, MRCGP, MRCP (Paediatrics), DCH
Le Dr Colin Tidy est un médecin du NHS, basé dans l'Oxfordshire.
À propos du critiqueVoir la biographie complète

Dr Hayley Willacy, FRCGP
Médecin généraliste, Auteur médical
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Le Dr Hayley Willacy était médecin généraliste au NHS travaillant dans le nord-ouest de l'Angleterre, qui a pris sa retraite de la pratique clinique en 2022 après 30 ans.
Historique de l'article
Les informations sur cette page sont rédigées et examinées par des cliniciens qualifiés.
Article également disponible en Anglais, Allemand, Espagnol, Français, Italien, Portugais, Hindi, Hébreu, Arabe, and Suédois.
Prochaine révision prévue : 14 mars 2028
16 mars 2023 | Dernière version

Demandez, partagez, connectez-vous.
Parcourez les discussions, posez des questions et partagez vos expériences sur des centaines de sujets de santé.

Vous ne vous sentez pas bien ?
Évaluez vos symptômes en ligne gratuitement
Inscrivez-vous à la newsletter Patient
Votre dose hebdomadaire de conseils de santé clairs et fiables - rédigés pour vous aider à vous sentir informé, confiant et maître de la situation.
En vous abonnant, vous acceptez notre Politique de confidentialité. Vous pouvez vous désabonner à tout moment. Nous ne vendons jamais vos données.
Plus sur les os, les articulations et les muscles
- Spondylarthrite ankylosante
- Spondyloarthrite axiale
- Bisphosphonates
- Côtes cassées ou contusionnées
- Chondrocalcinose
- Luxation
- Blessures et fractures de l'avant-bras
- Ganglion
- Blessure aux ischio-jambiers
- remplacement de la hanche
- Douleur articulaire
- Douleur lombaire
- Sclérose en plaques
- dystrophie musculaire
- Bursite olécrânienne
- Ostéomyélite
- Prévenir l'ostéoporose induite par les stéroïdes
- Arthrite psoriasique
- Rhabdomyosarcome
- Épicondylite latérale