Les déchirures méniscales
Des blessures au cartilage du genou
Revu par Dr Hayley Willacy, FRCGP Dernière mise à jour par Dr Colin Tidy, MRCGPDernière mise à jour 10 fév 2023
Respecte les directives éditoriales
- TéléchargerTélécharger
- Partager
- Language
- Discussion
- Version audio
- Ajouter aux sources préférées sur Google
Dans cette série :les blessures sportivesBlessure aux ischio-jambiersÉlongation de l'aineBlessure à la chevilleEntorses et fouluresblessures des ligaments du genou
Vous avez tous vu le footballeur à la télévision - un instant, il court à toute allure, l'instant d'après, il trébuche sur un autre joueur et se tient le genou en agonie. Il y a de fortes chances qu'une blessure au cartilage du genou soit au moins une partie du problème.
En un coup d'œil
Une blessure au cartilage du genou affecte le tissu conjonctif résistant recouvrant les os ou les ménisques absorbant les chocs.
Les symptômes peuvent inclure la douleur, le gonflement et le blocage du genou.
Le diagnostic implique souvent un examen physique et une IRM.
Le traitement initial comprend PRICE (Protection, Repos, Glace, Compression, Élévation) et éviter HARM.
Les analgésiques comme le paracétamol peuvent aider.
La physiothérapie est souvent recommandée pour renforcer les muscles du genou et favoriser la guérison.
La chirurgie peut être envisagée si les symptômes sont persistants ou sévères.
For some people, the symptoms of meniscal injury go away on their own after a few weeks. However, for other people the symptoms persist long-term, or flare up from time to time, until the tear is treated.
What are the symptoms of damaged articular cartilage?
It is much less common to damage your articular cartilage than it is to damage your meniscal cartilage (a meniscal tear). If you do injure your articular cartilage, it is very likely that you have also injured another part of your knee at the same time, such as one of the ligaments or your meniscus.
The symptoms that you get from any other injury may be more noticeable than the symptoms that are being caused by the injury to the articular cartilage.
Articular cartilage does not contain any nerves or blood vessels but you may still feel pain from a damaged articular cartilage. If it is painful, the pain tends to be felt around the joint line and on movement.
'Locking' of the knee can occur if a piece of cartilage affects the smooth movement of the knee.
The knee may swell and it may be painful to weight bear.
The knee joint
Cross-section diagram of the knee
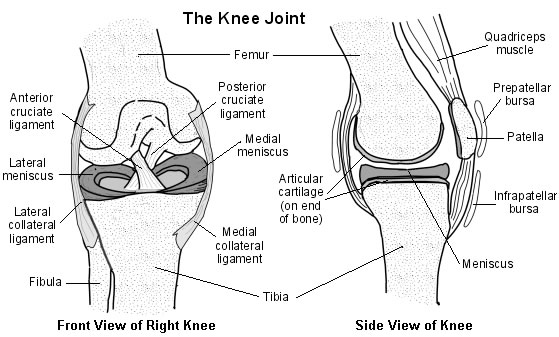
There are four bones around the area of the knee joint: the thigh bone (femur), the main shinbone (tibia), the outer shinbone (fibula) and the kneecap (patella). The main movements of the knee joint are between the femur, the tibia and the patella. Tough connective tissue (articular cartilage) covers the ends of the tibia and femur and the back of the patella around the knee joint. The articular cartilage reduces friction between the bones of the knee joint and helps smooth movement between them.
Each knee joint also contains an inner and outer meniscus (a medial and lateral meniscus). The menisci (plural of meniscus) are thick rubbery pads of cartilage tissue. They are C-shaped and become thinner towards the middle of the joint. The meniscal cartilages sit on top of, and are in addition to, the usual thin layer of articular cartilage which covers the top of the tibia. The menisci act like shock absorbers to absorb the impact of the upper leg on the lower leg. They also help to make the knee movements smooth and help to make the knee stable.
When people talk about a cartilage injury to a knee, they usually mean an injury to one of the menisci. However, the knee also has tough connective tissue covering the ends of the bones in the joint - this is called articular cartilage - and damage can occur here as well. The areas of articular cartilage can be seen in the side view of the knee joint in the diagram above.
How do you tear your meniscal cartilage?
The knee is commonly injured in sports, especially rugby, football and skiing. You may tear a meniscus by a forceful knee movement whilst you are weight bearing on the same leg. The typical injury is for a footballer to twist (rotate) the knee whilst the foot is still on the ground - for example, whilst dribbling around a defender.
Another example is a tennis player who twists to hit a ball hard but with the foot remaining in the same position. The meniscus tears fully or partially. How serious the injury is depends on how much is torn and the exact site of the tear.
Meniscal tears may also occur without a sudden severe injury. In some cases a tear develops due to repeated small injuries to the cartilage or to wear and tear (degeneration) of the meniscal cartilage in older people. In severe injuries, other parts of the knee may also be damaged in addition to a meniscal tear. For example, you may also sprain or tear a ligament.
Meniscal cartilage does not heal very well once it is torn. This is mainly because it does not have a good blood supply. The outer edge of each meniscus has some blood vessels but the area in the centre has no direct blood supply. This means that although some small outer tears may heal in time, larger tears, or a tear in the middle, tend not to heal.
How do you injure the articular cartilage?
Damage to the cartilage covering the end of the bones at the knee joint is called a chondral injury. If the underlying bone itself is also damaged, this is called an osteochondral injury.
Injuries to the articular cartilage usually happen in combination with other injuries to the knee, either to the meniscus (as above) or the knee ligaments or bones.
How is a meniscal tear diagnosed?
How you injured your knee and the symptoms you are getting may be enough to tell a doctor that you have a meniscal tear.
A doctor or therapist will need to examine your knee. Certain features of the examination may point towards a meniscal tear. They will also want to examine the rest of your leg, including your hip, to check for other injuries or other causes of your symptoms.
Cartilage doesn't show up well on an X-ray so an radiographie of your knee is not usually necessary. The one time you might need to have an X-ray would be if your doctor is concerned that you might have damaged your bone (rather than cartilage) when you injured your knee.
Knee ultrasound is limited compared with ultrasound for other joints because the cruciate ligaments and knee cartilages are usually difficult to see properly.
The diagnosis of a meniscal tear can be confirmed by a imagerie par résonance magnétique (IRM).
Computerised tomography (CT) scanning is not as good as an MRI for diagnosing a meniscal tear.
How is damage to the articular cartilage diagnosed?
Just as when someone injures their meniscal cartilage, the history of how you injured your knee is important. Examination of the knee may reveal a swelling of the joint (effusion), a 'crunching' of the joint (crepitus) or locking but these things can be caused by other conditions too. X-rays are sometimes useful but an IRM provides doctors with the best pictures of the articular cartilages of the knee.
Damage to your articular cartilage may be found on an MRI scan when you are having the scan for another reason. Your doctor may have requested the scan to investigate other injuries to your knee, such as a meniscal tear or a ligament injury.
Can I treat a knee cartilage injury myself?
For the first 48-72 hours think of:
PRICE - Protect, Rest, Ice, Compression, Tlevation; et
Do no HARM - no médicament antagoniste des récepteurs Heat, Deslcohol, Running or Massage.
PRICE:
Protect your injured knee from further injury.
Rest your affected knee for 48-72 hours following injury. Consider the use of crutches to keep the weight off your injured knee. However, many doctors say that you should actually not keep your injured knee immobile for too long. You can usually start some exercises to help keep your knee joint moving and mobile. Start these as soon as you can tolerate the exercises without them causing too much pain. You can ask your doctor when you can start to move your knee joint and what exercises you should do.
Ice should be applied as soon as possible after your knee injury - for 10-30 minutes. Less than 10 minutes has little effect. More than 30 minutes may damage the skin. Make an ice-pack by wrapping ice cubes in a plastic bag or towel. (Do not put ice directly next to skin, as it may cause ice-burn.) A bag of frozen peas is an alternative. Gently press the ice-pack on to your injured knee. The cold from the ice is thought to reduce blood flow to the damaged ligament. This may limit pain and inflammation. After the first application, some doctors recommend reapplying for 15 minutes every two hours (during daytime) for the first 48-72 hours. Do not leave ice on while asleep.
Compression with a bandage will limit swelling and will help to rest your knee joint. A tubular compression bandage can be used. Mild pressure that is not uncomfortable or too tight and does not stop blood flow is ideal. A pharmacist will advise on the correct size. Remove before going to sleep. You may be advised to remove the bandage for good after 48 hours. This is because the bandage may limit movement of the joint which should normally be moving more freely after this time. However, bandages of the knee are sometimes kept on for longer to help keep swelling down and to keep the affected knee more comfortable. Ask your health professional what is best in your case.
Tlevation aims to limit and reduce any swelling. For example, keep your foot on the affected side up on a chair with a pillow under your knee when you are sitting. It may be easier to lie on a sofa and to put your foot on some cushions. When you are in bed, put your foot on a pillow. The aim is that your affected knee should be above the level of your heart.
R is sometimes added to this list to make PRICER. R stands for Rehabilitation which is the most important part of the treatment for meniscal tears - to get you and your knee back to normal. You may need to see a physiotherapist or sports therapist for advice about exercises to do to strengthen and stretch the muscles around your knee if your symptoms persist.
(Remarque: despite the common guidance of putting an ice-pack on injuries, there is some evidence from animal studies that it can delay healing and some researchers in the field suggest the evidence base for putting ice on an injury should currently be thought of as equivocal.)
Avoid HARM for 72 hours after injury. That is, avoid:
médicament antagoniste des récepteurs Heat - for example, hot baths, saunas, heat packs. Heat has the opposite effect to ice on the blood flow. That is, it encourages blood flow. So, heat should be avoided when inflammation is developing. However, after about 72 hours, no further inflammation is likely to develop and heat may then be soothing.
Deslcoholic drinks, which can increase bleeding and swelling and decrease healing.
Running or any other form of exercise which may cause further damage.
Massage, which may increase bleeding and swelling. However, as with heat, after about 72 hours, gentle massage may be soothing.
What medication will help?
Paracetamol and codeine
Paracétamol is useful to ease pain. It is best to take paracetamol regularly, for a few days or so, rather than every now and then. An adult dose is two 500 mg tablets, four times a day. If the pain is more severe, you may be prescribed codéine, which is more powerful but can make some people drowsy and constipated.
Analgésiques anti-inflammatoires
These medicines are also called anti-inflammatoires non stéroïdiens (AINS). They relieve pain and may also limit inflammation and swelling. There are many types and brands. You can buy some (for example, aspirine et ibuprofène) at pharmacies, without a prescription. You need a prescription for others.
Side-effects sometimes occur with anti-inflammatory painkillers. Stomach pain, and bleeding from the stomach, are the most serious. Some people with asthme, l'hypertension artérielle, kidney failure, bad l'indigestion and heart failure may not be able to take anti-inflammatory painkillers. So, check with your doctor or pharmacist before taking them in order to make sure they are suitable for you.
Mais notez: The National Institute for Health and Care Excellence (NICE) Clinical Knowledge Summaries (CKS), a well-known source of guidance for doctors in the UK, do not recommend that anti-inflammatory painkillers be used in the first 48 hours after the injury. This is because of concerns that they may delay healing. The logic is that some inflammation is a necessary part of the healing process. So, it may be that decreasing inflammation too much by taking these medicines may impair the healing process. This is a supposed (theoretical) concern, as no trials have proved this point. Further research is needed to clarify the use of these medicines following an injury. Also, if you are having surgery to repair a torn ACL (see below), it is thought that, theoretically, NSAIDs may not be a good idea to take for a long period of time after the surgery because they may have an effect on the success of the surgery.
Rub-on (topical) anti-inflammatory painkillers
There are various types and brands of topical anti-inflammatory painkillers. You can buy some, without a prescription, at pharmacies. You need a prescription for the others. There is debate as to how effective rub-on anti-inflammatory painkillers are compared with tablets. Some studies suggest that they may be as good as tablets for treating sprains. Some studies suggest they may not be as good. However, the amount of the medication that gets into the bloodstream is much less than with tablets and there is less risk of side-effects.
Traitement supplémentaire
This will then depend on:
The severity of symptoms.
How any persisting symptoms are affecting your life.
Votre âge.
Votre santé générale.
When will you need physiotherapy for a meniscal tear and why?
Small tears may heal by themselves in time, usually over about six weeks. You may be advised to see a physiotherapist or sports therapist to advise you on how to strengthen the supporting structures of your knee, such as the quadriceps and hamstring muscles. Some tears don't heal but, even so, they may not cause long-term symptoms once the initial pain and swelling has settled, or cause only intermittent or mild symptoms. In these cases, no further treatment will be needed.
If you are having symptoms which interfere with your ability to work or which have been going on for more than 6-8 weeks, despite rehabilitation with a physiotherapist, a referral to an orthopaedic surgeon is advised. However, it is important to realise that if you have been diagnosed with a meniscal tear, even if it has shown up on an MRI scan, this doesn't mean you will have to have surgery.
If you do need surgery to your knee, you will be advised to have physiotherapy afterwards. This is so as to keep the knee joint active (which encourages healing) and to strengthen the surrounding muscles to give support and strength to the knee.
When will you need physiotherapy for an articular cartilage injury and why?
Advice from a physiotherapist can be particularly useful if you have been diagnosed with an articular cartilage injury. Moving the knee passively (which means moving it without using the surrounding muscles) may help the articular cartilage to heal. Moving the knee passively also helps to reduce the formation of scar tissue.
What operations are done for a meniscal tear?
If the tear causes persistent troublesome symptoms, particularly painful locking, then an operation may be advised - although evidence for the benefit of surgery is variable. Several studies have been done that suggest that surgical treatment for people who have a meniscal tear due to wear and tear (degeneration) is no better than following a standard exercise regime.
Most operations are done by arthroscopy (see below). The types of operations which may be considered include the following:
The torn meniscus may be able to be repaired and stitched back into place. However, in many cases this is not possible.
In some cases where repair is not possible, a small portion of the meniscus may be trimmed or cut out to even up the surface.
Sometimes, the entire meniscus is removed but this is rarely done as long-term results are not good.
Meniscal transplants have recently been introduced. The missing meniscal cartilage is replaced with donor tissue, which is screened and sterilised much in the same way as for other donor tissues such as for kidney transplants. These are more commonly performed in America than in Europe.
There is a new operation in which collagen meniscal implants are inserted. The implants are made from a natural substance and allow your cells to grow into it so that the missing meniscal tissue regrows. It is not yet known whether this is any better than other treatments.
What operations are done for damage to the articular cartilage?
The treatment of large injuries or those which cause persistent symptoms is by surgery. Surgery may involve a keyhole operation (arthroscopy - see below) to remove loose bits of cartilage or to transplant cartilage into the damaged area. Another method used to repair damaged knee cartilage is to make tiny holes (called microfractures) in the bone beneath the damaged cartilage. This releases bone marrow into the damaged cartilage. The bone marrow then helps to repair the cartilage. Unfortunately, the newly formed tissue can break down over time and long-term results may be disappointing. You may want to discuss the pros and cons of surgery and the type of surgery with your doctor.
If damaged articular cartilage that is bad enough to cause symptoms is left untreated, this may lead to early l'arthrose.
What is an arthroscopy?
This is a procedure that allows a surgeon to look inside a joint by using an arthroscope. An arthroscope is like a thin telescope with a light source. It is used to light up and magnify the structures inside a joint. Two or three small (less than 1 cm) cuts are made at the front of the knee. The knee joint is filled up with fluid and the arthroscope is introduced into the knee. Probes and specially designed tiny tools and instruments can then be introduced into the knee through the other small cuts. These instruments are used to cut, trim, take samples (biopsies), grab, etc, inside the joint. Arthroscopy can be used to treat meniscal tears and damaged articular cartilage. There are some risks from arthroscopy. See the separate leaflet called Arthroscopy and Arthroscopic Surgery for more details.
Following surgery, you will have physiotherapy to keep the knee joint active (which encourages healing) and to strengthen the surrounding muscles to give support and strength to the knee.
Sélections des patients pour les blessures sportives

Os, articulations et muscles
Blessure à la cheville
La cheville est une articulation complexe et elle est souvent blessée. Presque la moitié des blessures résultent de la pratique de sports ou d'exercices. Une entorse de la cheville est la blessure sportive la plus courante.
par Dr Hayley Willacy, FRCGP

Os, articulations et muscles
Entorses et foulures
A sprain is an injury to the band (ligament) which connects two or more bones to a joint. A sprain is usually caused by the joint being forced suddenly outside its usual range of movement. A severe sprain may look and feel like a break (fracture), and it can be difficult for health professionals to tell the difference between the two. A strain refers to an overstretching and tearing of muscles or tendons. Following a sprain or strain the usual advice is to pay the PRICE (Protection, Rest, Ice, Compression, and Elevation) and avoid HARM (Heat, Alcohol, Running, and Massage) for the first 48-72 hours after injury. Most sprains and strains heal within a few weeks. Note: this leaflet does not advise on how to distinguish what injury you have. For example, it is sometimes difficult to tell if you have a bone fracture, or other more serious injury. Therefore, see a doctor or nurse if you suspect that you have a fracture or other more serious injury. This leaflet assumes you know that you have a sprain or strain (for example, having been told by a doctor or nurse) and nothing more serious.
par Dr Doug McKechnie, MRCGP
Questions fréquemment posées
Quelle est la probabilité qu'une déchirure du ménisque guérisse naturellement ?
Les petites déchirures, en particulier celles situées sur le bord extérieur où il y a un apport sanguin, peuvent guérir d'elles-mêmes, souvent en environ six semaines. Cependant, les déchirures plus importantes ou celles situées dans la partie centrale du ménisque, qui manque d'un apport sanguin direct, ont tendance à ne pas bien guérir.
Y a-t-il des exercices ou activités spécifiques à éviter si j'ai une blessure du cartilage articulaire ?
Bien que l'article mentionne de protéger votre genou et de le reposer pendant 48 à 72 heures après une blessure, il déconseille également l'immobilité prolongée. Vous devriez commencer quelques exercices pour garder votre genou en mouvement dès que vous pouvez les tolérer sans douleur excessive. Il est recommandé de demander à votre médecin ou physiothérapeute quels exercices spécifiques sont appropriés et quelles activités éviter pour prévenir d'autres dommages.
Est-il toujours nécessaire de subir une intervention chirurgicale si une IRM confirme une déchirure méniscale ?
Non, un diagnostic de déchirure méniscale sur une IRM ne signifie pas automatiquement que vous aurez besoin d'une chirurgie. De nombreuses déchirures, même si elles ne guérissent pas, peuvent ne pas causer de symptômes persistants à long terme une fois que la douleur et le gonflement initiaux se sont atténués. Dans ces cas, aucun traitement supplémentaire peut ne pas être nécessaire, surtout si la rééducation avec un physiothérapeute est efficace.
Combien de temps devrai-je utiliser des béquilles après une blessure au cartilage du genou ?
Pour les premières 48 à 72 heures après une blessure, vous pouvez envisager d'utiliser des béquilles pour ne pas mettre de poids sur votre genou blessé. Cependant, de nombreux médecins suggèrent d'éviter l'immobilité prolongée. Vous devriez discuter avec votre médecin ou physiothérapeute du moment approprié pour cesser l'utilisation des béquilles et commencer à bouger.
Que se passe-t-il si une lésion du cartilage articulaire endommagé n'est pas traitée ?
Si le cartilage articulaire endommagé est suffisamment grave pour provoquer des symptômes et n'est pas traité, cela peut entraîner le développement précoce de l'arthrose du genou.
Puis-je appliquer de la chaleur sur mon genou après la phase initiale de blessure ?
La chaleur doit être évitée pendant les 72 premières heures suivant une blessure car elle favorise la circulation sanguine et peut aggraver l'inflammation. Cependant, après environ 72 heures, lorsque l'inflammation initiale est probablement résorbée, l'application de chaleur peut être apaisante.
Lectures complémentaires et références
- Bhan K; Meniscal Tears: Current Understanding, Diagnosis, and Management. Cureus. 2020 Jun 13;12(6):e8590. doi: 10.7759/cureus.8590.
- Beaufils P, Pujol N; Management of traumatic meniscal tear and degenerative meniscal lesions. Save the meniscus. Orthop Traumatol Surg Res. 2017 Dec;103(8S):S237-S244. doi: 10.1016/j.otsr.2017.08.003. Epub 2017 Sep 2.
- Stein JM, Yayac M, Conte EJ, et al; Treatment Outcomes of Meniscal Root Tears: A Systematic Review. Arthrosc Sports Med Rehabil. 2020 Apr 28;2(3):e251-e261. doi: 10.1016/j.asmr.2020.02.005. eCollection 2020 Jun.
- Karia M, Ghaly Y, Al-Hadithy N, et al; Current concepts in the techniques, indications and outcomes of meniscal repairs. Eur J Orthop Surg Traumatol. 2019 Apr;29(3):509-520. doi: 10.1007/s00590-018-2317-5. Epub 2018 Oct 29.
À propos de l'auteurVoir la biographie complète

Dr Colin Tidy, MRCGP
Médecin généraliste, Auteur médical
MBBS, MRCGP, MRCP (Paediatrics), DCH
Le Dr Colin Tidy est un médecin du NHS, basé dans l'Oxfordshire.
À propos du critiqueVoir la biographie complète

Dr Hayley Willacy, FRCGP
Médecin généraliste, Auteur médical
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Le Dr Hayley Willacy était médecin généraliste au NHS travaillant dans le nord-ouest de l'Angleterre, qui a pris sa retraite de la pratique clinique en 2022 après 30 ans.
Historique de l'article
Les informations sur cette page sont rédigées et examinées par des cliniciens qualifiés.
Article également disponible en Anglais, Allemand, Espagnol, Français, Italien, Portugais, Hindi, Hébreu, Arabe, and Suédois.
Prochaine révision prévue : 9 févr. 2028
10 fév 2023 | Dernière version

Demandez, partagez, connectez-vous.
Parcourez les discussions, posez des questions et partagez vos expériences sur des centaines de sujets de santé.

Vous ne vous sentez pas bien ?
Évaluez vos symptômes en ligne gratuitement
Inscrivez-vous à la newsletter Patient
Votre dose hebdomadaire de conseils de santé clairs et fiables - rédigés pour vous aider à vous sentir informé, confiant et maître de la situation.
En vous abonnant, vous acceptez notre Politique de confidentialité. Vous pouvez vous désabonner à tout moment. Nous ne vendons jamais vos données.