Polypes intestinaux
Colonic polyps
Revu par Dr Colin Tidy, MRCGPDernière mise à jour par Dr Toni Hazell, MRCGPLast updated 15 sept. 2023
Respecte les directives éditoriales
- TéléchargerTélécharger
- Partager
- Language
- Discussion
- Version audio
- Add to preferred sources on Google
Dans cette série :Cancer du côlonDépistage du cancer de l'intestinTest immunochimique fécalSigmoïdoscopieColoscopieColonoscan
Les polypes intestinaux (polypes du côlon) sont de petites excroissances non cancéreuses (bénignes) sur la muqueuse interne de l'intestin (côlon et rectum).
Dans cet article:
Video picks for Problèmes intestinaux
Continuez à lire ci-dessous
What are bowel polyps?
A bowel polyp is a small non-cancerous growth. There are many types of polyps, such as those that occur in the nose - this leaflet is about polyps that occur in the bowel.
Types of bowel polyps
Retour au sommaireLarge bowel - polyp
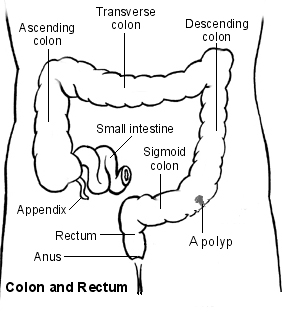
Most bowel polyps develop in the part of the colon called the descending colon, which leads down to the rectum. However, they can occur anywhere in the colon or rectum. Bowel polyps can be divided into three types: hyperplastic polyps, adenomas and polyposis syndromes.
Hyperplastic bowel polyps
These are a common type of bowel polyps. They are small - usually less than half a centimetre in diameter. They are generally regarded as harmless and only very rarely turn into cancer.
Adenomas
These too are a common type of bowel polyp. Most are small (usually less than a centimetre in diameter) but they can be bigger. There is a small risk that an adenoma may, in time, become cancerous. If one does turn cancerous, the change usually takes place after a number of years.
The relationship between polyps and cancer is that most bowel cancers (colorectal cancers) develop from a polyp that has been present for 5-15 years. In other words, although most adenomas do not become cancerous, the vast majority of cancers in the bowel initially develop from an adenoma that has been present for a number of years.
It is difficult to be certain of the exact risk of developing cancer from an adenoma. One study suggested that for a single 1 cm adenoma, the risk of it turning cancerous was about 1 in 12 after 10 years, and about a 1 in 4 after 20 years. However, the risk seems to vary depending on factors such as the size of the adenoma and the exact type of adenoma.
There are different types of adenoma and some types are more likely than others to develop into bowel cancer. See also the separate leaflet on Dépistage du cancer colorectal.
Polyposis syndromes
Polyposis syndromes are a group of inherited conditions. They include:
Familial adenomatous polyposis (FAP).
Hereditary nonpolyposis colorectal cancer (HNPCC)/Lynch's syndrome.
Gardner's syndrome.
Turcot's syndrome.
Peutz-Jeghers syndrome.
Cowden's disease.
Familial juvenile polyposis.
Hyperplastic polyposis.
These are rare syndromes. They cause polyps in young people and often cause multiple bowel polyps that have a high chance of developing into bowel cancer.
Continuez à lire ci-dessous
Bowel polyp symptoms
Retour au sommaireMost people with one or more bowel polyps do not have any symptoms. Most people who have a bowel polyp will never know they have one.
However, some people with bowel polyps will get symptoms. Polyps do not usually cause abdominal pain or a change in bowel habits. Symptoms include:
Blood in the stools (faeces). There may also be mucus in the stools.
Diarrhée ou constipation, but this is much less likely than blood in the stools. Diarrhoea or constipation is much more likely to have a cause other than a bowel polyp.
Causes of bowel polyps
Retour au sommaireThe lining of the bowel constantly renews itself throughout our lives. New cells are made in the lining of the bowel and these cells eventually die to be replaced by more new cells. Each of these cells contains genes which control how the cell works.
Family history may play a role, because if the gene doesn't work properly then some cells may grow more quickly. This may eventually cause a polyp to develop. Some faulty genes cause a tendency for the lining of the bowel to develop polyps or bowel cancer, which may be inherited from our parents.
Continuez à lire ci-dessous
How common are bowel polyps?
Retour au sommaireBowel polyps are really common in older people. About 1 in 4 people over the age of 50 years develop at least one colonic polyp. Bowel polyps are much less common in younger people.
Some people develop just one bowel polyp. It is not uncommon to have two or more. However, having more than five polyps is unusual.
Facteurs de risque
Risk factors include increasing age, being overweight and smoking. If you have a family history of a bowel polyp or cancer, or have had either of these yourself in the past, you are also at higher risk. Another risk factor is having inflammatory bowel disease (ulcerative colitis or Crohn's disease).
Diagnosing bowel polyps
Retour au sommaireMost bowel (colonic) polyps do not cause symptoms. So, most people with bowel polyps will not be diagnosed. Screening tests may be done if you have symptoms that indicate a bowel problem, or for various other reasons. For example, if you have seen blood in your stools (faeces) or if you are found to have blood in your stools following a routine screening test which is now offered to older people.
See the separate leaflet called Faecal Occult Blood Test for more details.
Qu'est-ce qu'une coloscopie ?
Most bowel polyps are diagnosed by this procedure. Colonoscopy is a test where an operator - a doctor or a nurse - looks into your colon. A colonoscope is a thin, flexible telescope. It is about as thick as a little finger. It is passed through the anus and into the colon. It can be pushed all the way around the colon as far as the caecum (where the small and large intestine meet). The colonoscope contains fibre-optic channels which allow light to shine down so the operator can see inside your colon.
See the separate leaflet called Colonoscopy for more details.
A sample (biopsy) will be taken at the time of the colonoscopy. This is very important so that it can be checked whether the polyp is cancerous (malignant).
What about other tests?
Sometimes a bowel polyp is diagnosed by other tests:
A special X-ray test of the bowel - this procedure is called a barium enema.
A CT colonogram - air and a contrast dye are pumped into the bowel to make the anatomy clearer to see and you are then examined by a CT scanner.
A test procedure called sigmoidoscopy - this enables a doctor or nurse to use an instrument called a sigmoidoscope to look into the rectum and sigmoid colon. The procedure is similar to a colonoscopy but it uses a shorter telescope.
If a bowel polyp is seen on a barium enema or CT colonogram you will still need a colonoscopy to remove the polyp and to take a sample (biopsy) of it for further investigation. The advantage of a colonoscopy as the first test is that the biopsy can be taken and/or the polyp removed all at the same time.
You will also need a colonoscopy if a polyp is found when you have a sigmoidoscopy. This is to make sure there are no more polyps beyond the reach of sigmoidoscopy.
Treatments for bowel polyps
Retour au sommaireIf you are diagnosed with a bowel polyp, you will usually be advised to have it removed, even if it is not causing any symptoms. This is because there is a small risk of the polyp developing into a cancerous (malignant) growth at some time in the future.
Coloscopie
Most bowel polyps can be removed during a colonoscopy. The colonoscope has a side channel down which a grabbing device can be passed. This device can be manipulated by the operator. The operator can therefore see and also remove a polyp during a colonoscopy. The removal of the polyp is usually painless. Once removed, the bowel/colon polyp is sent to the laboratory to be looked at under a microscope. This is done to check:
That it has been completely removed.
The type of polyp.
Whether it is non-cancerous (benign) or showing signs of cancerous (malignant) change.
Most removed polyps will show full removal and be totally benign.
Your consultant will advise on the need for follow-up. This may depend on factors such as the size of the bowel polyp, the exact type of polyp that has been removed, the laboratory report about the polyp, and your age. Once these factors are considered, some people are advised to have regular colonoscopies in the future to make sure no more bowel polyps develop. As with any test, the results should be given to you by the team who arranged the test. So if you are not sure about how to access the results, phone or email your consultant's secretary, not your GP.
Chirurgie
If you have many bowel polyps (especially if you have a polyposis syndrome) then you may need to have an operation to remove part of your bowel. This is because it isn't possible to completely remove all the bowel polyps by using colonoscopy.
Preventing bowel polyps
Retour au sommairePolyps cannot be prevented, but a healthy lifestyle (not smoking and not being overweight) can help to reduce your risk.
Patient picks for Problèmes intestinaux

Santé digestive
Diverticules
Les diverticules du côlon sont courants chez les personnes âgées, mais aussi chez les jeunes. Ils ne provoquent généralement aucun symptôme, et dans la plupart des cas, aucun traitement n'est nécessaire. Cependant, un régime riche en fibres est généralement conseillé pour aider à prévenir les complications. Dans certains cas, les diverticules provoquent des douleurs et d'autres symptômes. Parfois, un diverticule peut saigner et entraîner un saignement soudain et indolore par l'anus, qui peut être abondant. Dans certains cas, un ou plusieurs diverticules deviennent infectés, provoquant une diverticulite. Cela peut entraîner une douleur abdominale intense et une fièvre. Un traitement par antibiotiques peut être nécessaire. Les complications causées par la diverticulite — telles qu'une collection de pus (abcès) ou une perforation de l'intestin — sont rares, mais graves.
par Dr Philippa Vincent, MRCGP

Santé digestive
Ulcère duodénal
Un ulcère duodénal est généralement causé par une infection par un germe (bactérie) appelé Helicobacter pylori (H. pylori). Un traitement de 4 à 8 semaines avec un médicament antiacide permettra à l'ulcère de guérir. De plus, un traitement d'une semaine avec deux antibiotiques plus un médicament antiacide éliminera généralement l'infection à H. pylori. Cela empêche généralement l'ulcère de revenir. Les médicaments anti-inflammatoires utilisés pour traiter des affections telles que l'arthrite provoquent parfois des ulcères duodénaux. Il serait très inhabituel qu'une personne ayant un ulcère duodénal connu reçoive un médicament anti-inflammatoire, mais s'il n'y a absolument aucune alternative, il peut être administré avec un traitement antiacide à long terme.
par Dr Toni Hazell, MRCGP
Lectures complémentaires et références
- Combined endoscopic and laparoscopic removal of colonic polyps; NICE Interventional procedures guidance, September 2014
- Colorectal cancer (management in people aged 18 and over); NICE Guidance (2020, last updated December 2021)
- Bowel screening; NICE CKS, May 2019 (UK access only)
- Bonnington SN, Rutter MD; Surveillance of colonic polyps: Are we getting it right? World J Gastroenterol. 2016 Feb 14;22(6):1925-34. doi: 10.3748/wjg.v22.i6.1925.
Continuez à lire ci-dessous
About the authorView full bio

Dr Toni Hazell, MRCGP
MBBS, BSc, MRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
Dr. Toni Hazell qualified from St. Mary’s Hospital Medical School and did her VTS at Northwick Park Hospital.
About the reviewerView full bio

Dr Colin Tidy, MRCGP
Médecin généraliste, Auteur médical
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
Historique de l'article
Les informations sur cette page sont rédigées et examinées par des cliniciens qualifiés.
Prochaine révision prévue : 13 sept. 2028
15 sept. 2023 | Dernière version

Demandez, partagez, connectez-vous.
Parcourez les discussions, posez des questions et partagez vos expériences sur des centaines de sujets de santé.

Vous ne vous sentez pas bien ?
Évaluez vos symptômes en ligne gratuitement
Inscrivez-vous à la newsletter Patient
Votre dose hebdomadaire de conseils de santé clairs et fiables - rédigés pour vous aider à vous sentir informé, confiant et maître de la situation.
By subscribing you accept our Politique de confidentialité. Vous pouvez vous désabonner à tout moment. Nous ne vendons jamais vos données.