
Que se passe-t-il lors d'une crise d'asthme ?
Revu par Dr Hayley Willacy, FRCGP Dernière mise à jour par Dr Laurence KnottDernière mise à jour 24 avr. 2019
Respecte les directives éditoriales
- TéléchargerTélécharger
- Partager
- Language
- Discussion
- Version audio
- Ajouter aux sources préférées sur Google
L'asthme est une affection courante qui affecte les petites voies respiratoires (bronchioles). De temps en temps, les voies respiratoires se rétrécissent chez les personnes asthmatiques. Les symptômes typiques sont la respiration sifflante, la toux, la sensation d'oppression thoracique et l'essoufflement. L'ampleur du rétrécissement, ainsi que la durée de chaque épisode, peuvent varier considérablement.
The normal respiratory system
To understand what happens in asthme you need to be familiar with the normal breathing (respiratory) system and how the lungs and airways are arranged.
Normally, air entering through the mouth and nose travels through the main airway (the trachea) through a series of smaller branching airways called bronchi. The bronchi divide up into even smaller airways called bronchioles, which end in millions of tiny air sacs called alveoli.
When air enters the alveoli, the oxygen it contains passes through the thin membrane covering each sac into surrounding blood vessels. The oxygen attaches itself to red blood cells which then circulate around the body, releasing the oxygen into the body tissues.
Que se passe-t-il lors d'une crise d'asthme ?
An asthma attack starts with exposure to an asthma trigger. Triggers that cause an asthma attack vary from person to person but may be something you are allergic to such as animals or pollen. They can also be viral infections, reflux gastro-œsophagien, air pollution, cigarette smoke, and niveaux de stress.
When exposed to a trigger factor, the lining of the airways responds by producing chemicals such as histamine and leukotriene. These chemicals are in part responsible for the changes that happen in the lungs during an asthma attack.
The airway lining becomes inflamed and swells. The production of mucus, normally present in a small amount in the airways, is increased. Typically this results in throat clearing, spitting up phlegm (sputum) and coughing. The muscles wrapped round the bronchioles eventually become constricted or tightened (bronchospasm) and the air passing through the narrowed channels produces a wheeze.
Lungs and alveoli
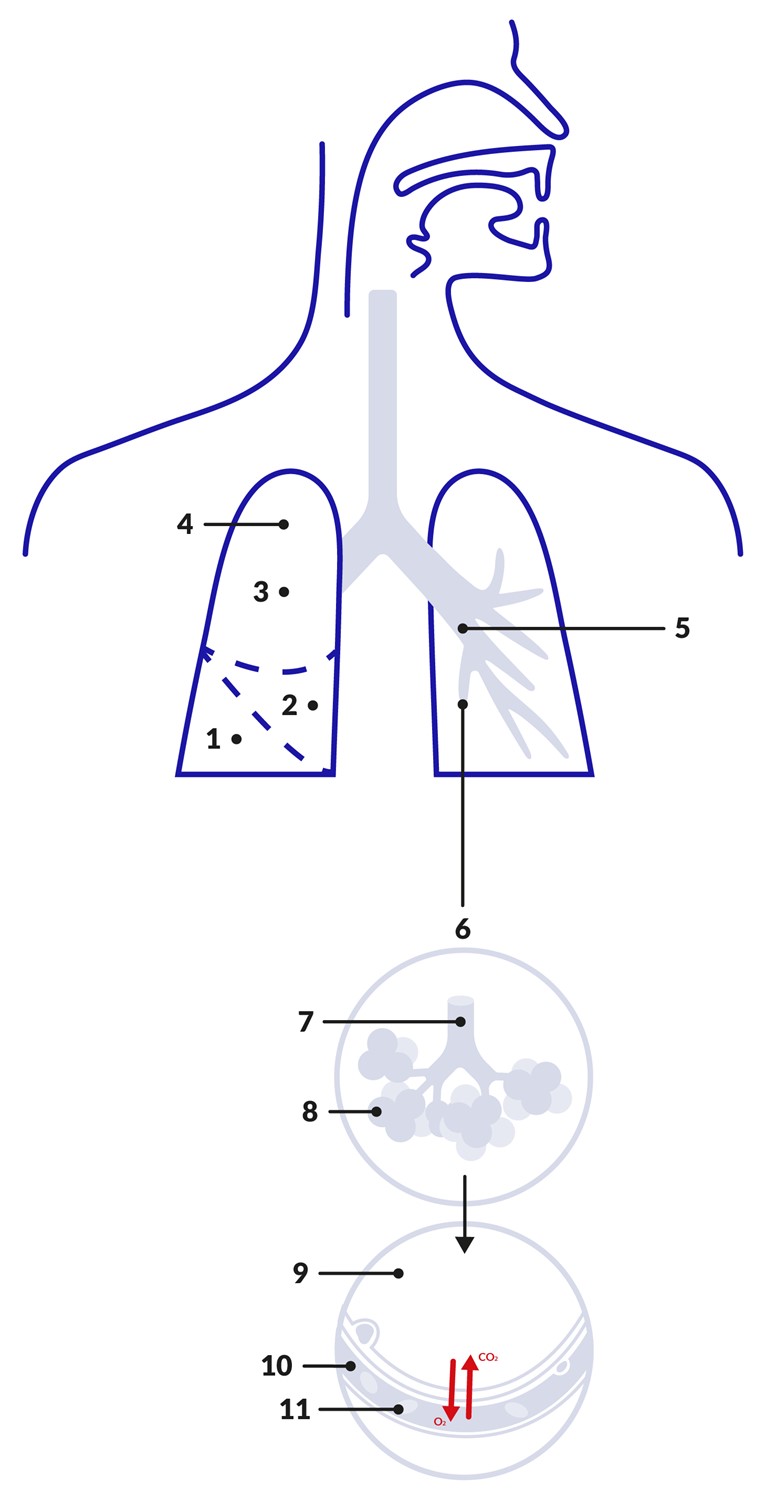
Key | |
|---|---|
1. Lower lobe | 7. Terminal bronchiole |
Cross-section of normal airway
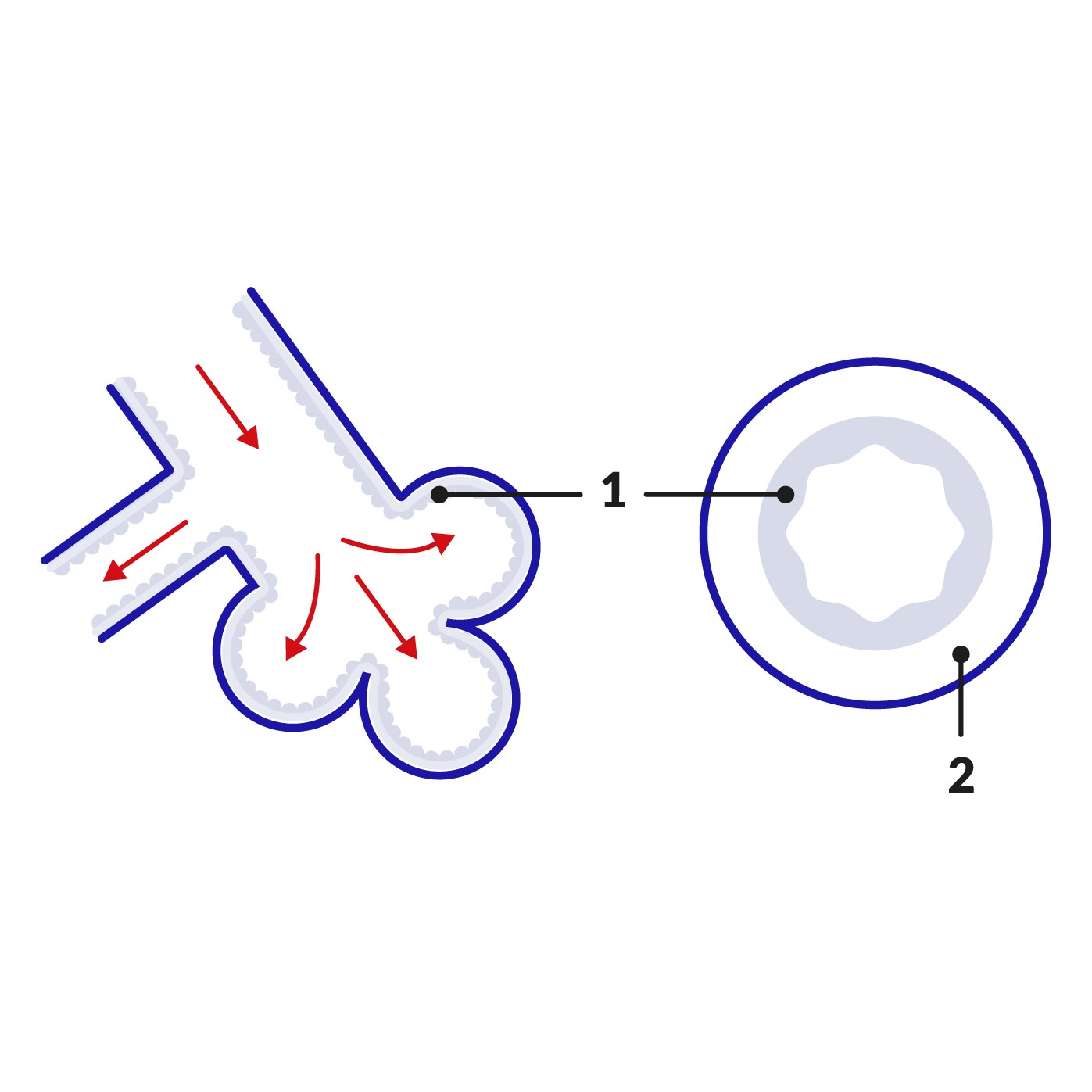
Key |
|---|
1. Small amount of mucus lines the airways |
Cross-section of airway during asthma attack
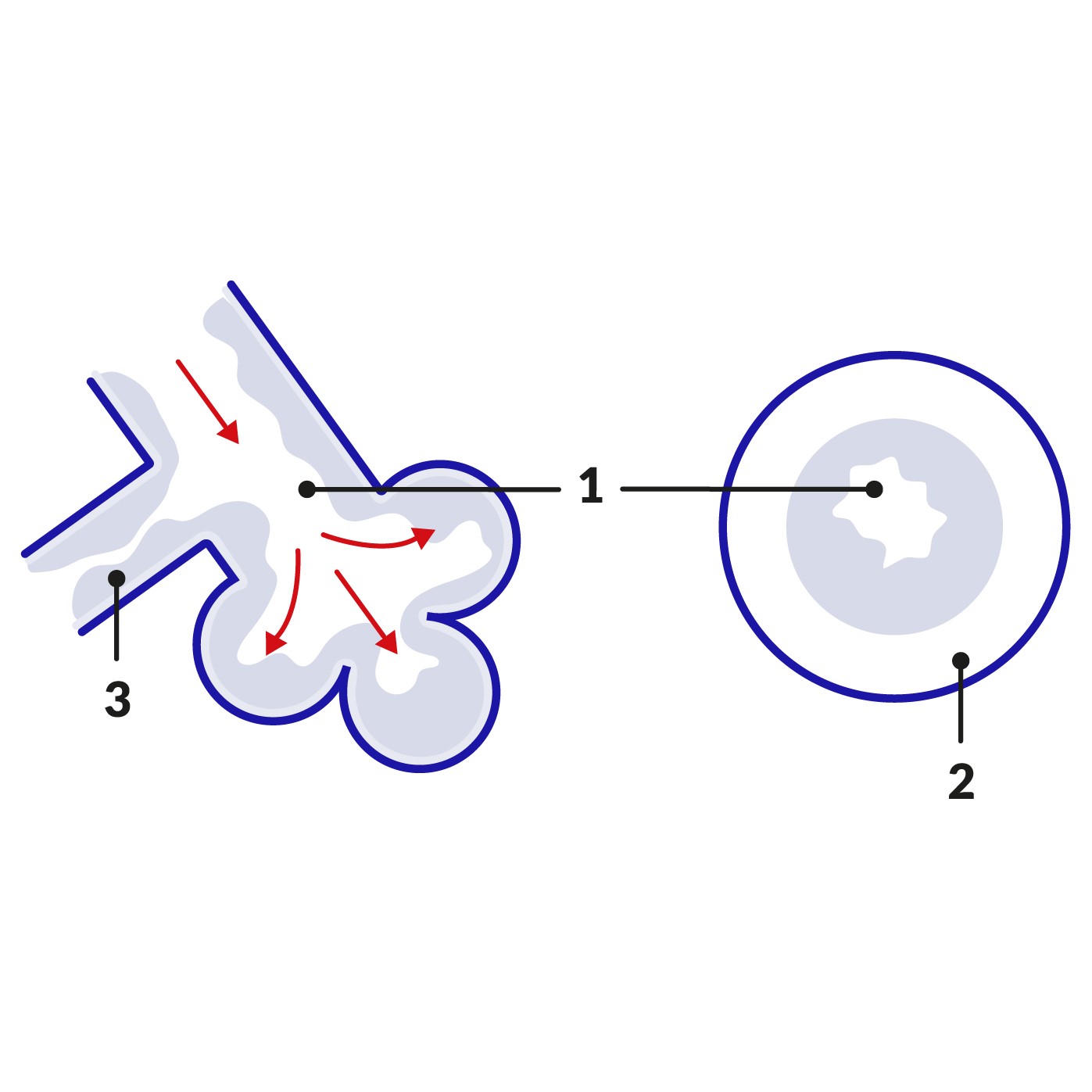
Key |
|---|
1. Reduced flow of air to the alveoli |
So you can see there are three reasons why people who are having an asthma attack become breathless. The swelling of the lining of the airways, the increased mucus production and the bronchospasm all result in less air than normal entering the alveoli. There is therefore a limited amount of oxygen available to pass on to the red blood cells.
Why asthma treatments work
Bronchodilators
Bronchodilators such as salbutamol work by relaxing the muscle of the bronchioles and widening the channels through which the air passes. They are usually administered in the form of inhalers. Salbutamol starts to work within a few minutes and the effect will last between 3-5 hours. Bronchodilator inhalers are referred to as 'reliever' inhalers or 'blue' inhalers. This is because they relieve symptoms of breathlessness, and the inhalers are usually blue in colour. Although they relieve breathlessness, they do not prevent the breathlessness from happening.
Salmeterol works in a similar way to salbutamol but its effects last for about 12 hours.
Corticostéroïdes
Steroids such as beclometasone work by reducing the inflammation in your airways. When the inflammation has gone, your airways are much less likely to become narrow and cause symptoms such as wheezing. For asthma, steroids are usually prescribed in inhaler form. Although they have no effect during acute asthma attacks, when taken regularly (usually twice daily) they are the inhalers that will stop the attacks from happening. They are usually brown in colour and are known as 'preventer' or 'brown' inhalers. Occasionally, for severe asthma, steroids are prescribed in tablet form.
If your asthma stabilises on steroid and bronchodilator inhalers your doctor may prescribe a combination inhaler to take regularly which contains both medicines.
Autres traitements
Antileukotrienes
Antileukotrienes such as montélukast act by blocking the action of leukotriene. Leukotriene is produced when people with asthma come into contact with trigger factors such as substances they are allergic to (such as pollen), or exercise. Leukotriene causes the lining of the bronchioles to become inflamed and swollen and antileukotrienes help to prevent this. Not every person with asthma gets a significant rise in leukotriene production during an attack, which is why antileukotrienes are usually kept in reserve for asthma which does not respond to standard bronchodilator and steroid therapy.
Omalizumab
Omalizumab is a medicine that is only given by injection. It works by interfering with the immune system to reduce inflammation in the airways which is present in asthma. It is reserved for people with severe asthma who do not respond to standard treatment. It can only be started by a specialist.
Sélections des patients pour Asthme

Poitrine et poumons
Quelles sont les principales causes de l'asthme et des crises d'asthme ?
L'asthme est une affection pulmonaire chronique dont environ 12 % de la population britannique a été diagnostiquée, selon la British Lung Foundation. Bien que certaines personnes souffrant d'asthme pendant l'enfance finissent par en guérir, d'autres nécessitent une gestion continue à l'âge adulte. La bonne nouvelle est qu'il existe des moyens de mieux gérer l'asthme et d'améliorer considérablement la qualité de vie de quelqu'un.
par Amberley Davis

Poitrine et poumons
Comment fonctionnent les inhalateurs ?
Millions of us use inhalers in the UK. For some, they're a lifesaver. For others, they provide welcome relief. For others still, they're more of a security blanket to be carried around in the bottom of your bag just in case.
par Josh Alderman
À propos de l'auteurVoir la biographie complète

Dr Laurence Knott
Médecin généraliste, Auteur médical
Licence (Hons) Biochimie, MBBS
Le Dr Laurence Knott a obtenu son diplôme en 1973 et a acquis une vaste expérience en tant que médecin généraliste.
À propos du critiqueVoir la biographie complète

Dr Hayley Willacy, FRCGP
Médecin généraliste, Auteur médical
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Le Dr Hayley Willacy était médecin généraliste au NHS travaillant dans le nord-ouest de l'Angleterre, qui a pris sa retraite de la pratique clinique en 2022 après 30 ans.
Historique de l'article
Les informations sur cette page sont examinées par des cliniciens qualifiés.
Article également disponible en Anglais, Allemand, Espagnol, Français, Italien, Portugais, Hindi, Hébreu, Arabe, and Suédois.
24 avr. 2019 | Dernière version

Demandez, partagez, connectez-vous.
Parcourez les discussions, posez des questions et partagez vos expériences sur des centaines de sujets de santé.

Vous ne vous sentez pas bien ?
Évaluez vos symptômes en ligne gratuitement
Inscrivez-vous à la newsletter Patient
Votre dose hebdomadaire de conseils de santé clairs et fiables - rédigés pour vous aider à vous sentir informé, confiant et maître de la situation.
En vous abonnant, vous acceptez notre Politique de confidentialité. Vous pouvez vous désabonner à tout moment. Nous ne vendons jamais vos données.
Plus dans la poitrine et les poumons
- Suis-je en train de faire une crise cardiaque ?
- Les décès dus à l'asthme en Angleterre et au Pays de Galles au plus haut depuis une décennie
- Un nouveau test sanguin peut-il détecter le cancer du poumon précocement ?
- Peut-on vraiment 'guérir' de l'asthme en grandissant ?
- Comment éviter d'attraper un rhume dans les transports en commun
- Comment gérer l'asthme pendant les mois d'hiver
- Comment vivre sainement avec la BPCO
- Comment gérer la BPCO en hiver
- Est-ce la coqueluche ou juste un rhume ?
- Le cancer du poumon chez les non-fumeurs est plus courant que vous ne le pensez
- Gérer le rhume des foins et l'asthme : conseils pour survivre à la saison pollinique
- Les parents doivent-ils s'inquiéter de la 'noyade sèche' ?
- Devriez-vous aller travailler lorsque vous avez un rhume ?
- Le système respiratoire
- Quels sont les différents types d'inhalateurs pour l'asthme ?
- Quelles sont les étapes du cancer du poumon ?
- Qu'est-ce que le HMPV et devons-nous nous en inquiéter ?
- Qu'est-ce qui cause votre douleur thoracique ?
- Quand s'inquiéter d'une toux persistante
- Pourquoi la pollution de l'air est-elle si dangereuse pour vos poumons ?