Stérilisation féminine
Revu par Dr Hayley Willacy, FRCGP Dernière mise à jour par Dr Toni Hazell, MRCGPLast updated 19 mai 2023
Respecte les directives éditoriales
- TéléchargerTélécharger
- Partager
- Language
- Discussion
- Version audio
- Add to preferred sources on Google
Dans cette série :StérilisationVasectomie
La stérilisation féminine est une méthode de contraception. C'est une procédure réalisée pour empêcher les ovules d'atteindre les spermatozoïdes.
At a glance
Female sterilisation blocks the Fallopian tubes to prevent eggs from reaching sperm.
The procedure usually takes about 20 minutes and is often done as a day-case.
It is a permanent method of contraception with a failure rate of 0.5 per cent.
Recovery from keyhole surgery usually takes a few days, but longer for open surgery.
There is a small risk of ectopic pregnancy if sterilisation fails.
Female sterilisation does not protect against sexually transmitted infections.
Dans cet article:
Video picks for Other surgery and procedures
Continuez à lire ci-dessous
How is female sterilisation done?
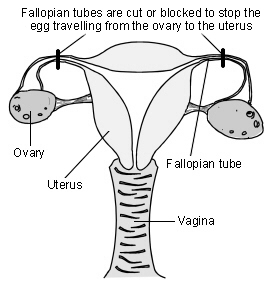
The tubes between the ovary and the womb (the Fallopian tubes) are cut or blocked with rings or clips. This stops the eggs which are released by the ovary from reaching the sperm.
Organes reproducteurs féminins
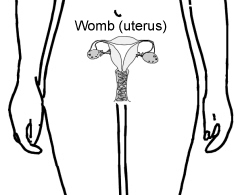
Diagram showing how female sterilisation is performed
The operation is usually done under general anaesthetic but can be done with a local or regional anaesthetic while you are awake. For most women the operation is done with the help of a special telescope called a laparoscope.
The laparoscope is inserted through a very small cut in your tummy (abdomen). It allows the surgeon to see what they are doing. Another small cut is then made to insert an instrument to block the tubes. A number of ways are used to do this. Most often clips or rings are applied to your tubes. The clips or rings provide a block in the tubes and prevent the egg from meeting sperm.
A larger cut may have to be made, and a more traditional operation done, in some women. This is more likely if laparoscopie is too risky, such as if you have had multiple previous operations, or if you are overweight. This is called a mini-laparotomy.
If blocking the Fallopian tubes doesn't work then either part or all of the tubes can be removed. This is called a salpingectomy.
Sterilisation can be performed at the same time as a césarienne, when a segment of the tube is removed. This is done after the delivery of the baby. It has a higher failure rate than a sterilisation which is not done at the time of caesarean delivery.
How long does the procedure take?
The procedure itself usually takes about 20 minutes, and should be done as a day-case, so you arrive at hospital early in the morning and go home the same day (unless there are unexpected complications).
How reliable is female sterilisation?
Retour au sommaireThe failure rate of female sterilisation is 0.5%, so 1 in 200 women will get pregnant within one year As a comparison, when no contraception is used, more than 800 out of 1,000 sexually active women will become pregnant within one year. This failure rate is much higher than for some long-acting reversible contraceptive (LARC) methods (for example only 1 woman in 2000 will get pregnant per year on the implant) and so a LARC should always be offered to a woman who is considering sterilisation.
After sterilisation, women can become pregnant if the tubes come back together again after being cut. If clips were used to block the tubes, the clips can occasionally work their way off - even when they have been put on correctly.
Continuez à lire ci-dessous
Advantages of female sterilisation
Retour au sommaireDo you still have periods after being sterilised?
It is permanent and you (and your partner) don't have to think about contraception again. There are no hormones involved, so you do not have the side-effects of many other types of contraception.
Disadvantages of female sterilisation
Retour au sommaireSterilisation is permanent and very difficult to reverse. Some women may regret having the operation in future years, particularly if their circumstances change. Periods may become heavier after sterilisation - sometimes this is because you have stopped using another method, such as the pill, which lightens your periods, but it can also happen if you have not moved from another method.
In the rare event that the procedure fails and you become pregnant, you are more likely to have an grossesse extra-utérine. This occurs when the pregnancy develops outside of the womb, usually in the Fallopian tube. You would need emergency treatment if this were to happen. If you think you are pregnant after a sterilisation, or have unexplained bleeding or pain in your tummy (abdomen), then see a doctor quickly.
Laparoscopic sterilisation is also not as easy to do or as effective as male sterilisation (vasectomy). There is a small risk from the insertion of the laparoscope which has to be done 'blind' (ie without any image guidance). This means the surgeon cannot see exactly where they are putting the instrument in the tummy to gain access to the tubes.
It may at times damage organs like bowel or a blood vessel inside the abdomen. This sounds worrying. However, the surgeon takes many precautions to make the procedure safe and to avoid causing damage to any other organ and, in most cases, this does not happen.
Sterilisation doesn't protect against sexually transmitted infection (STIs) so you may need to use condoms if you think you may be at risk of STI.
As with any operation there is a risk of a wound infection and the slight risk from a general anaesthetic. There may be some tummy discomfort or bloating, or mild discomfort or pain at the site of the cut.
Continuez à lire ci-dessous
How soon is female sterilisation effective?
Retour au sommaireFor laparoscopic sterilisation it depends on when you have it done in your menstrual cycle. If it is done whilst you have your period, you will not have produced an egg yet. In this case the procedure is effective immediately.
At any other time in your cycle, you will usually be advised to continue your previous method of contraception until your next period.
(The procedure is only done after checking you are not pregnant. That is, a pregnancy test would be done. If you have had sex without using contraception in the previous three weeks it is not possible to be sure you will not be pregnant. In this case, the operation would be delayed.)
Does female sterilisation affect sex drive?
Retour au sommaireNo. Sex may seem more enjoyable, as the worry of pregnancy and contraception is removed.
How long does it take to recover from female sterilisation?
Retour au sommaireIt usually takes a few days to recover from a laparoscopic sterilisation and most people can return to work within five days, but should avoid heavy lifting for a week. If a mini-laparotomy (open surgery rather than keyhole) was needed then recovery will be longer, and you may need to be off work for 3-4 weeks and avoid heavy lifting for 6 weeks. It is always important to care for yourself after surgery.
Points to consider
Retour au sommaireDon't consider having the operation unless you and your partner are sure you do not want children, or further children. It is wise not to make the decision at times of crisis or change - for example, after a new baby or termination of pregnancy. Don't make the decision if there are any major problems in your relationship with your partner. It will not solve any sexual problems.
Doctors normally like to be sure that both partners are happy with the decision before doing this permanent procedure. However, it is not a legal requirement to get your partner's permission. If you have any doubts and questions, make sure you discuss these with your doctor or practice nurse.
Have you considered the alternatives? Female sterilisation is not 100% effective. Other reversible methods of contraception are often more effective, such as the système intra-utérin (SIU), contraceptive implants et contraceptive injections. Also, male sterilisation is easier and safer to do and is more effective.
Patient picks for Other surgery and procedures

Chirurgie et procédures
Chirurgie thoracoscopique assistée par vidéo
La chirurgie thoracoscopique assistée par vidéo (VATS) est une procédure chirurgicale qui permet aux médecins de voir à l'intérieur de la poitrine et des poumons. C'est une forme de chirurgie 'mini-invasive' qui peut être utilisée pour réaliser différentes interventions chirurgicales. Remarque : les informations ci-dessous sont une simple indication générale. Les modalités et la façon dont les examens sont effectués peuvent varier d'un hôpital à l'autre. Suivez toujours les instructions données par votre médecin ou votre hôpital local.
par Dr Laurence Knott

Chirurgie et procédures
Vasectomie
La vasectomie est une méthode de contraception où un homme subit une petite opération pour couper l'extrémité du canal déférent. C'est le tube qui transporte les spermatozoïdes des testicules (testicules) vers le pénis. Les spermatozoïdes sont produits dans les testicules. Une fois le canal déférent coupé, les spermatozoïdes ne peuvent plus entrer dans le sperme qui est éjaculé lors des rapports sexuels. La vasectomie est très fiable - mais pas tout à fait à 100 %. Même après une opération réussie, environ 1 homme sur 2 500 ayant subi une vasectomie redeviendra fertile à un moment donné dans le futur. Cela est dû au fait que, rarement, les deux extrémités du canal déférent coupé se rejoignent à nouveau avec le temps.
par Dr Philippa Vincent, MRCGP
Questions fréquemment posées
What is the main purpose of female sterilisation?
Female sterilisation aims to prevent pregnancy by cutting or blocking the Fallopian tubes. This action stops eggs released from the ovaries from reaching sperm, thereby preventing fertilisation.
Are there different ways the Fallopian tubes can be blocked during sterilisation?
Yes, there are several methods. Most commonly, clips or rings are applied to your Fallopian tubes to create a block. In some cases, if blocking isn't effective or suitable, part or all of the tubes can be removed, a procedure known as a salpingectomy.
Can sterilisation be performed at the same time as a caesarean section?
Yes, female sterilisation can be done immediately after the delivery of a baby during a caesarean section. In this scenario, a segment of the Fallopian tube is removed. However, it's worth noting that sterilisations performed at this time have a higher failure rate compared to those done separately.
What happens if sterilisation fails and a woman becomes pregnant?
If sterilisation fails and you become pregnant, there is a higher risk of an ectopic pregnancy. This is where the pregnancy develops outside the womb, usually in the Fallopian tube, and requires emergency medical treatment. You should see a doctor quickly if you suspect pregnancy or experience unexplained bleeding or pain in your tummy after sterilisation.
Why is female sterilisation considered less easy or effective than male sterilisation?
Laparoscopic female sterilisation is not as easy to perform or as effective as male sterilisation (vasectomy). There's also a small risk associated with inserting the laparoscope 'blindly', which means without direct visual guidance, potentially damaging internal organs like bowel or blood vessels. Surgeons take precautions to minimise these risks, but they are factors to consider.
How soon after the procedure can I resume my normal activities?
Most women recover from a laparoscopic sterilisation within a few days and can return to work within five days. However, it's advised to avoid heavy lifting for about a week. If a mini-laparotomy (open surgery) was required, recovery takes longer, potentially needing 3-4 weeks off work and avoiding heavy lifting for 6 weeks.
Does female sterilisation protect against sexually transmitted infections?
No, female sterilisation only prevents pregnancy. It does not offer any protection against sexually transmitted infections (STIs). If you believe you are at risk of STIs, you would still need to use barrier methods like condoms.
Lectures complémentaires et références
- Trussell J; Échec contraceptif aux États-Unis, Contraception, 2011
- Stérilisation masculine et féminine; Faculté de Santé Sexuelle et Reproductive (septembre 2014)
- Contraception - sterilization; NICE CKS, mai 2021 (accès réservé au Royaume-Uni)
Continuez à lire ci-dessous
About the authorView full bio

Dr Toni Hazell, MRCGP
MBBS, BSc, MRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
Dr. Toni Hazell qualified from St. Mary’s Hospital Medical School and did her VTS at Northwick Park Hospital.
About the reviewerView full bio

Dr Hayley Willacy, FRCGP
Médecin généraliste, Auteur médical
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr Hayley Willacy was an NHS GP working in northwest England, who retired from clinical practice in 2022 after 30 years.
Historique de l'article
Les informations sur cette page sont rédigées et examinées par des cliniciens qualifiés.
Prochaine révision prévue : 12 mai 2028
19 mai 2023 | Dernière version

Demandez, partagez, connectez-vous.
Parcourez les discussions, posez des questions et partagez vos expériences sur des centaines de sujets de santé.

Vous ne vous sentez pas bien ?
Évaluez vos symptômes en ligne gratuitement
Inscrivez-vous à la newsletter Patient
Votre dose hebdomadaire de conseils de santé clairs et fiables - rédigés pour vous aider à vous sentir informé, confiant et maître de la situation.
By subscribing you accept our Politique de confidentialité. Vous pouvez vous désabonner à tout moment. Nous ne vendons jamais vos données.