Macrocytose et anémie macrocytaire
Revu par Dr Rosalyn Adleman, MRCGPDernière mise à jour par Dr Philippa Vincent, MRCGPDernière mise à jour 3 juin 2025
Respecte les directives éditoriales
- TéléchargerTélécharger
- Partager
- Language
- Discussion
- Version audio
- Ajouter aux sources préférées sur Google
Dans cette série :AnémieRégimes adaptés aux personnes souffrant d'anémieCarence en acide foliqueAnémie ferripriveCarence en vitamine B12 et anémie pernicieuse
La macrocytose se réfère à des globules rouges qui sont plus grands que la normale. Elle ne cause pas de symptômes en elle-même.
En un coup d'œil
Macrocytosis is when red blood cells are larger than normal.
It can be a sign of low vitamin B12 or folic acid levels.
Macrocytosis itself does not cause symptoms, but macrocytic anaemia does.
Symptoms of macrocytic anaemia include breathlessness, tiredness, and a 'thumping' heart.
Vitamin B12 deficiency can also cause nervous system problems like pins and needles.
Causes include certain medicines, alcohol, and deficiencies in vitamin B12 or folic acid.
Treatment for macrocytosis involves addressing the underlying cause or deficiency.
Macrocytosis symptoms
You may also find relevant information in our other separate leaflet called What is blood?
Macrocytosis can exist without anaemia. Macrocytosis itself does not cause any symptoms but can be a sign of low levels of other vitamins such as vitamin B12 or folic acid.
Macrocytic anaemia causes the same symptoms as with any other kind of l'anémie. In mild macrocytic anaemia you may not get any symptoms. You're more likely to notice symptoms if you are older or have coronary heart disease. Younger people can sometimes be quite anaemic without noticing any problems at all.
Symptoms you may notice include:
Symptômes de une insuffisance cardiaque.
Si vous avez angine de poitrine, you may notice your chest pains getting worse.
If your macrocytic anaemia is due to carence en vitamine B12 you may also notice nervous system problems such as pins and needles, numbness, vision changes and unsteadiness. If it is severe, you may also develop depression or confusion. Normally these symptoms only develop if the deficiency is severe and has been untreated for a long time.
If the anaemia is severe, a doctor examining you may notice that you:
Look paler than normal (the nails, eyes and tongue are a good place to check).
Have a bounding pulse (a pulse which feels stronger and more powerful than normal).
Have signs of une insuffisance cardiaque.
Have a heart murmur between the left second and third ribs when the heart is contracting (a pulmonary flow murmur).
In mild-moderate anaemia there are often very few signs on examination.
Causes of macrocytosis
Macrocytosis can be caused by:
Medicines such as azathioprine.
Depending on the severity and how long the person has had the condition, some of these causes can eventually lead to anaemia.
There are two types of macrocytic anaemia:
Megaloblastic macrocytic anaemia
Non-megaloblastic macrocytic anaemia
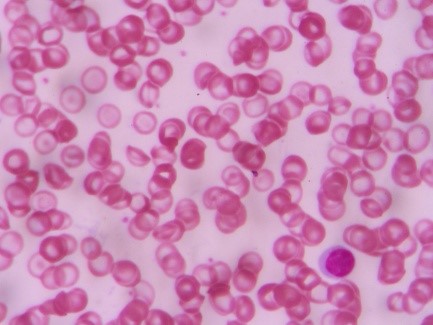
The difference is in the presence or absence of megaloblasts. These are large, abnormally developed red blood cells visible when a pathologist uses a microscope to look at a slide smeared with blood.
Causes of megaloblastic macrocytic anaemia include:
Serum B12 deficiency (when associated with a low haemoglobin, this is often called anémie pernicieuse, although actually pernicious anaemia is only one of the causes of vitamin B12 deficiency).
Surgery that removes a part of the stomach (gastrectomy) or part of the gut called the ileum (ileal resection), causing difficulty in absorbing vitamin B12 from the diet.
Infection of the gut with germs (bacteria) or parasites (organisms that live in the body and obtain nutrition from it).
Deficiency of vitamin B12 in the diet - this can happen in strict vegans but even then it is rare.
Carence en acide folique. This can be due to:
Not eating enough foods containing folic acid. Foods high in folic acid include broccoli, Brussels sprouts, asparagus, peas, chickpeas and brown rice.
Medical conditions affecting the gut - for example, maladie cœliaque.
Inflammatory conditions such as maladie de Crohn.
Some blood disorders can lead to a very high turnover of red blood cells - for example, la drépanocytose et thalassémie. Normal amounts of folic acid in the diet may then not be enough and supplements may need to be taken.
Some medicines interfere with folic acid. Therefore, you may need to take extra folic acid whilst taking certain medicines. These include colestyramine, sulfasalazine, méthotrexate et quelques anticonvulsant medicines used to treat epilepsy. If you need dialysis then you may be recommended to take folic acid supplements.
Causes of non-megaloblastic macrocytic anaemia include:
Alcohol use over the recommended limits.
Maladie du foie.
Severe underactivity of the thyroid gland (hypothyroïdie).
An increase in the number of immature red blood cells called reticulocytes (reticulocytosis).
Other blood disorders including myeloid leukaemia, aplastic anaemia (a condition affecting the bone marrow) and some other rare blood conditions.
Medicines that affect how the genetic material DNA is produced, such as azathioprine.
How are macrocytosis and macrocytic anaemia diagnosed?
These conditions will show up on a blood film. Your doctor may have arranged this test as part of a routine check or because you have felt unwell (see the section on symptoms, above). Once the condition has been diagnosed, further tests will be arranged to find the cause. You may also need tests to check whether you have any conditions that people who have macrocytosis or macrocytic anaemia frequently develop.
The tests may include:
A reticulocyte count. This may be raised if there is a rapid turnover of red blood cells - for example, in conditions in which red cells are destroyed, such as haemolytic anaemia. If you're found to have such a condition, more tests (for example, a Test de Coombs) may be needed to investigate the cause.
The level of folate in your blood.
The level of serum B12 in your blood.
Tests of your liver function.
Checks to rule out conditions which people with some types of macrocytic anaemia develop, such as diabetes, underactive thyroid gland, and homocystinuria (a condition in which a chemical called homocysteine and related substances build up in the blood and urine).
If some rare blood disorders are suspected, you may need a bone marrow examination, but this is the exception rather than the rule.
Other tests may be needed if your doctor suspects other conditions need to be ruled out.
Macrocytosis treatment
If it has been identified that your macrocytosis is caused by a deficiency, this will need to be treated, whether or not you have anaemia.
You will also need treatment for the condition that caused the deficiency in the first place.
Traditionally with vitamin B12 deficiency, people were offered an injectable form of the vitamin called hydroxocobalamin. Your practice nurse will usually inject this into a muscle every 3-6 months.
However, it is more common nowadays for you to be prescribed B12 tablets (cyanocobalamin) first. These do not work as well as the injections if the B12 deficiency is due to difficulties with absorption but can work well where vitamin B12 deficiency is due to a lack of vitamin B12 in the diet. This used to be rare but is becoming more common.
If you have folic acid deficiency you will be advised to take des comprimés d'acide folique. 5 mg daily for four months is usually advised.
If you have vitamin B12 and folic acid deficiency together, it's important that the B12 deficiency be treated first, otherwise, a rare but serious spinal cord complication (subacute combined degeneration of the cord) can occur.
Treatment of the underlying cause will depend on the condition. For example, if your deficiency was due to excessive use of alcohol, this will need to be addressed.
Sélections des patients pour Anémie
Allergies, sang et système immunitaire
Carence en acide folique
Un régime équilibré normal contient suffisamment d'acide folique. Cependant, une carence en acide folique peut provoquer une anémie et parfois d'autres symptômes.
par Dr Rosalyn Adleman, MRCGP
Allergies, sang et système immunitaire
Drépanocytose
Sickle cell disease (SCD) is a serious, inherited condition affecting the blood and various organs in the body. It affects the red blood cells, causing episodes of 'sickling', which produce episodes of pain and other symptoms. In between episodes of sickling, people with SCD are normally well. Long-term complications can occur. Good treatment, started early in life, can prevent complications. So, early diagnosis and specialist treatment are advised for SCD. Sickle cell trait is not the same as sickle cell disease.
par Dr Hayley Willacy, FRCGP
Questions fréquemment posées
Are macrocytes dangerous?
Macrocytosis, which means having larger-than-normal red blood cells (macrocytes), is not dangerous in itself. It is a sign that there might be an underlying condition that needs to be investigated, such as low levels of vitamins like B12 or folic acid. The danger comes from the underlying cause or if macrocytosis leads to macrocytic anaemia.
What is megaloblastic macrocytic anaemia?
Megaloblastic macrocytic anaemia is a specific type of macrocytic anaemia. It is distinguished by the presence of 'megaloblasts', which are abnormally developed large red blood cells. These cells can be seen when a pathologist examines a blood sample under a microscope. Common causes include vitamin B12 deficiency (sometimes called pernicious anaemia) and folic acid deficiency.
How do doctors check for conditions related to macrocytosis?
Once macrocytosis or macrocytic anaemia is diagnosed through a blood film, your doctor will arrange further tests to find the cause and to check for any related conditions. These tests might include measuring levels of folate and serum B12 in your blood, checking liver function, and ruling out conditions like diabetes, underactive thyroid, or homocystinuria. In rare cases, if certain blood disorders are suspected, a bone marrow examination might be needed.
Lectures complémentaires et références
- Anémie - Carence en B12 et en folates; NICE CKS, mars 2024 (accès réservé au Royaume-Uni)
À propos de l'auteurVoir la biographie complète

Dr Philippa Vincent, MRCGP
Médecin généraliste, Auteur médical
MB BS, Bsc, MRCGP (2000), DCH, DFSRH, DRCOG
Dr Philippa Vincent est un médecin généraliste du NHS travaillant dans le nord de Londres.
À propos du critiqueVoir la biographie complète

Dr Rosalyn Adleman, MRCGP
MRCGP
Dr Rosalyn Adleman est médecin généraliste du NHS travaillant dans le nord de Londres.
Historique de l'article
Les informations sur cette page sont rédigées et examinées par des cliniciens qualifiés.
Article également disponible en Anglais, Allemand, Espagnol, Français, Italien, Portugais, Hindi, Hébreu, Arabe, and Suédois.
Prochaine révision prévue : 2 juin 2028
3 juin 2025 | Dernière version
9 Jul 2017 | Publié à l'origine

Demandez, partagez, connectez-vous.
Parcourez les discussions, posez des questions et partagez vos expériences sur des centaines de sujets de santé.

Vous ne vous sentez pas bien ?
Évaluez vos symptômes en ligne gratuitement
Inscrivez-vous à la newsletter Patient
Votre dose hebdomadaire de conseils de santé clairs et fiables - rédigés pour vous aider à vous sentir informé, confiant et maître de la situation.
En vous abonnant, vous acceptez notre Politique de confidentialité. Vous pouvez vous désabonner à tout moment. Nous ne vendons jamais vos données.